


Table of Contents
Traumatic Brain Injury and Posture: Why Balance, Alignment, and Integrative Care Matter

Overview
Traumatic brain injuries can change the way a person stands, walks, and holds their body. After a mild TBI or concussion, many people notice that their balance feels “off” for weeks or months. They may sway more, feel dizzy in busy environments, or struggle on soft surfaces. In severe TBIs, the body can take on rigid reflex postures—decorticate or decerebrate posturing—that signal a medical emergency and require immediate care (call emergency services). These problems occur because brain injury can disrupt the systems that maintain our balance: vision, sensory/proprioceptive input from joints and muscles, and the vestibular system (inner ear balance organs). It can also involve the neck and upper back, where spinal alignment affects head position, eye-head reflexes, and body orientation.
This article explains:
-
How mild and severe TBIs change posture and balance
-
What decorticate and decerebrate posturing look like and why they matter
-
Why symptoms such as headaches and dizziness can worsen with cervical and upper thoracic misalignments
-
How an integrated care plan—including chiropractic adjustments, vestibular and sensory-motor therapies, and nurse-practitioner oversight—can support recovery
-
Which tests and tools help diagnose TBI-related balance and posture problems, listed from simple to advanced
-
Practical, step-by-step tips you can bring to your care team
Mild TBI: Subtle but Real Changes in Postural Control
Even when a concussion looks “mild” on day one, changes in posture and balance can linger. Research shows that individuals with a history of mild TBI (mTBI) demonstrate altered postural dynamics compared with those without prior mTBI, indicating that control of body sway and balance strategies can remain different long after symptoms should have resolved (Sosnoff et al., 2011). PMC
People often describe this as feeling “unstable,” “on a boat,” or “wobbly” on uneven ground. These sensations can appear in busy supermarkets, while scrolling on a phone, or while walking in the dark. Community resources also reflect how common this is: 30–65% of people with brain injuries report having balance problems, emphasizing how widespread and persistent these issues can be. braininjurycanada.ca
Why does it happen:
-
Sensory mismatch. The brain blends three information streams—vision, vestibular input, and proprioception. After TBI, the weighting between them can be off.
-
Delayed processing or slower reaction times. Even small delays can change how you correct a stumble.
-
Cervical (neck) contributions. Neck muscles and joint receptors feed the brain position information; if the neck is stiff, painful, or misaligned after a crash or fall, balance can worsen. A review highlights cervical spine involvement in concussion-related symptoms and the value of addressing neck dysfunction as part of care (Morin et al., 2016). PMC
Severe TBI: Abnormal Posturing Is an Emergency
After severe brain injury or major disruption of brain function, some patients may take on reflex, rigid postures that signal serious brain damage.
-
Decorticate posturing: arms flexed and drawn to the chest; legs extended and rigid. It indicates major brain injury or disruption and is a red-flag emergency. Cleveland Clinic+1
-
Decerebrate posturing: arms and legs rigidly extended with the head and neck arched back; often considered more ominous and linked to damage in the lower midbrain/pons. Immediate medical attention is required. Cleveland Clinic+1
If you ever notice these patterns, call emergency services immediately. These postures are part of coma assessments (for example, with the Glasgow Coma Scale) and reflect a critical state of the nervous system. Cleveland Clinic+1
How TBI Disrupts the “Balance Triad”
We stay upright by fusing three systems:
-
Vision: what you see
-
Vestibular: inner ear organs sensing head motion and position
-
Proprioception: body feedback from muscles, joints, and skin
TBI can scramble any one or all three. Damage to brain networks that process these signals leads to dizziness, unsteadiness, and poor postural control (Row et al., 2019). PMC
Common postural signs after mTBI
-
Increased sway when standing still
-
Trouble with head turns or busy visual environments
-
Feeling “pulled” to one side
-
Difficulty walking while turning the head or looking around
-
More falls or near-falls when fatigued
Objective studies show that reactive balance responses (the quick steps you take to catch yourself) can remain impaired even in athletes who have cleared, supporting the idea that return-to-play decisions should consider balance reactions, not just symptoms. Frontiers
Cervical and Upper Thoracic Links: Why Alignment Matters
Concussions and whiplash often happen together. The cervical spine is a dense hub of sensors that tell your brain where your head is in space. If the neck is injured, stiff, or misaligned, the brain may receive distorted signals, which can drive dizziness, headaches, and poor postural control. A review of neck involvement in mTBI states that while high-quality evidence is still developing, clinical experience and emerging studies support assessing and treating cervical dysfunction alongside concussion care (Morin et al., 2016). PMC
What this means for posture:
-
Forward-head or guarded neck posture can change the center of mass and increase sway.
-
Cervical joint restriction can disrupt head-eye-neck coordination, causing dizziness when scanning your surroundings.
-
Upper thoracic stiffness limits rib and shoulder motion, which can alter breathing mechanics and the subtle trunk movements used to maintain balance.
Symptoms That Tie Posture and TBI Together
-
Headaches that worsen by the end of the day or with screen time
-
Dizziness/vertigo when turning the head, rolling in bed, or walking in stores
-
Neck pain/stiffness and a tendency to hold the neck rigid
-
Fatigue with standing, grocery shopping, or long conversations
-
Anxiety/fear of falling, which can further stiffen posture and reduce natural sway
Across research and community organizations, balance problems are common after TBI and are influenced by many factors, including injury severity and medical complications. Model Systems research notes that poorer sitting/standing balance is associated with more severe injuries and longer rehabilitation stays, emphasizing the need for early balance assessment. Brain Injury Association of America
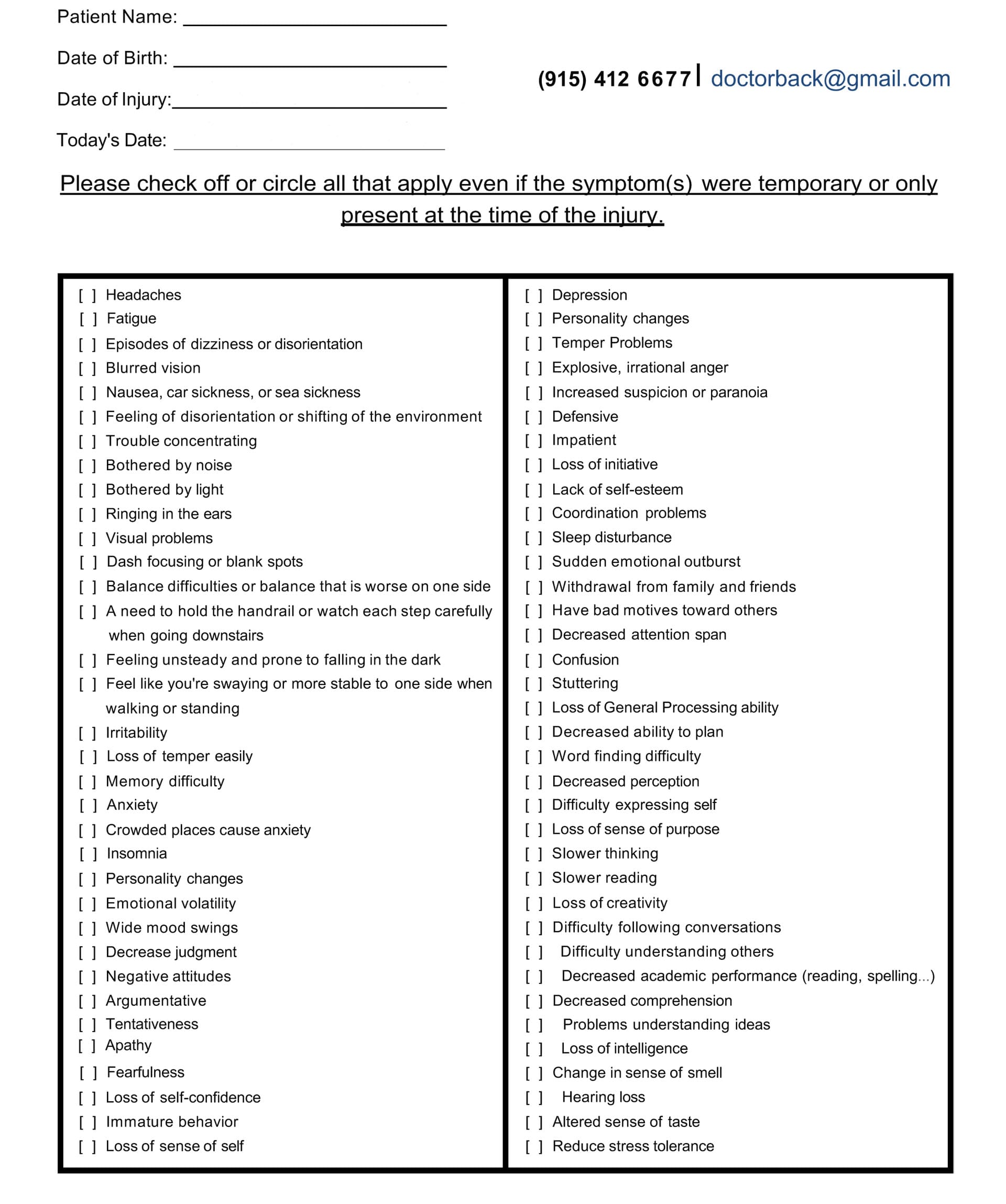
Symptom Questionnaire:
Abnormal Posturing vs. Postural Control Problems: Key Differences
| Feature | Mild TBI Postural Control Issues | Severe TBI Abnormal Posturing |
|---|---|---|
| Consciousness | Awake; symptoms fluctuate | Usually unconscious/coma |
| Appearance | Subtle sway, unsteady gait, head-eye coordination issues | Rigid reflex patterns (decorticate/decerebrate) |
| Trigger | Complex visual scenes, uneven surfaces, fatigue | Severe brain damage/disruption |
| Urgency | Outpatient assessment and rehab | Medical emergency—call 911 |
| Goal of care | Restore multi-sensory balance, integration, and cervical mobility | Stabilize patient; intensive neurocritical care |
How Integrative Chiropractic Care Can Help
Important: Chiropractic care does not replace emergency or primary medical management of TBI. It can be part of a comprehensive team approach that includes medical evaluation, vestibular/oculomotor rehabilitation, physical therapy, and cognitive support (education, pacing, sleep, nutrition). (General guidance echoed by multiple clinics and community resources.) Northwest Florida Physicians Group+1
1) Spinal adjustments to improve alignment and reduce neck-driven symptoms
When appropriate and applied with clinical screening, chiropractic adjustments can restore segmental motion, reduce joint irritation, and optimize afferent input from the cervical spine. This may ease cervicogenic headaches and neck-related dizziness and support balance work by improving head-neck mechanics (clinical reviews and practice guidance). PMC
2) Sensory-motor and vestibular therapies
Modern chiropractic practices that integrate functional neurology add targeted eye-head exercises, balance training, and graded sensory exposure to encourage neuroplasticity. These therapies aim to recalibrate the blending of vision, vestibular, and proprioception and improve reactive postural responses. HML Functional Care
3) Posture retraining and breathing mechanics
Improving rib mobility and diaphragmatic breathing helps reduce bracing patterns and restores normal postural sway rather than rigid “guarding,” which often worsens dizziness and fatigue.
4) Circulation and cerebrospinal fluid (CSF) considerations
Some integrative clinicians discuss optimizing cerebral perfusion and CSF movement indirectly by improving thoracic mobility, neck mechanics, and overall autonomic balance. While hard clinical trials are limited, clinicians—such as Dr. Alexander Jimenez—educate patients about cerebral perfusion pressure (CPP) and emphasize systemic factors (hydration, breathing, and sleep) that support brain blood flow and recovery. These concepts should be framed as adjunctive and theoretical benefits pending stronger evidence. El Paso, TX Doctor Of Chiropractic
5) Lifestyle and symptom management
Education on sleep, graded activity, nutrition, and stress regulation reduces symptom flare-ups and helps patients participate more fully in rehab—a theme repeated in clinical blogs and integrative practices. Impact Medical Group+1
Dr. Alexander Jimenez’s Clinical Observations (DC, APRN, FNP-BC)
Drawing from his dual scope as a chiropractor and nurse practitioner, Dr. Jimenez emphasizes:
-
Team-based care: Chiropractic treatment is coordinated with medical evaluation, imaging when indicated, and targeted rehab, rather than used alone.
-
Neck-brain connection: Following a concussion, a careful evaluation of cervical alignment and mobility is crucial, as it impacts headaches, dizziness, and posture.
-
Targeted rehab: Combining vestibular, proprioceptive, and postural exercises with spine care helps retrain the nervous system.
-
Patient education: Clear guidance on pacing, sleep, hydration, and nutrition supports nervous-system recovery and cerebral perfusion.
(For his educational materials on TBI and neurological recovery, see his clinical site and recent posts.) El Paso, TX Doctor Of Chiropractic+1
A Practical, Step-by-Step Care Plan
Always start with medical assessment if you’ve had a head injury, new neurologic symptoms, or worsening dizziness.
Step 1. Medical screening and risk check
-
Red flags: worsening headache, repeated vomiting, confusion, fainting, abnormal posturing, weakness, vision loss, seizures → emergency care. Cleveland Clinic+1
Step 2. Baseline balance and neck assessment
-
Stand with feet together, then heel-to-toe, eyes open/closed (with supervision)
-
Gentle range-of-motion of the neck; note pain and stiffness
-
Simple gait checks: head turns while walking, dual-task (count backwards while walking)
Step 3. Build a team
-
Nurse practitioner/physician for diagnosis, medication review, and referrals
-
Chiropractor for cervical/upper-thoracic mechanics and posture care
-
Vestibular therapist (PT/OT/functional neurology) for eye-head-balance retraining
-
Behavioral health and nutrition as needed
Step 4. Early, gentle inputs
-
Cervical mobility: gentle hands-on care and home mobility drills
-
Visual-vestibular: gaze stabilization (e.g., “VOR x1”), smooth pursuit, saccade drills as prescribed
-
Proprioception: weight shifting, ankle strategy training, stance on progressively challenging surfaces
Step 5. Progress to dynamic balance
-
Walking with head turns, obstacle navigation, reactive stepping, and sport-specific or job-specific drills
Step 6. Posture retraining during daily life
-
“Stacked” posture: ears over shoulders, gentle chin nod, ribs over pelvis
-
Micro-breaks for screens; breathing resets (4-second inhale, 6-second exhale)
-
Light strength work for deep neck flexors, scapular stabilizers, and hips
Diagnostic Tools: From Simplest to Most Advanced
Note: Exact testing should be chosen by qualified clinicians. This list helps you understand the pathway from simple screens to sophisticated assessments.
A. Bedside & clinic screens (simplest)
-
Symptom checklists & history (headache, dizziness, nausea, visual strain, brain fog)
-
Neurologic exam (cranial nerves, strength/sensation, reflexes)
-
Gait observation and Romberg/sharpened Romberg
-
Balance Error Scoring System (BESS) or similar simple stance tests
-
Cervical ROM and palpation; head-eye coordination checks
Evidence note: Bedside balance tests are easy to use, but can show ceiling effects (they may miss subtle deficits). More sensitive tools are often needed in TBI. Frontiers
B. Focused functional measures
-
Community Balance and Mobility Scale (CB&M) – detects higher-level balance and mobility issues in TBI better than basic scales like the Berg Balance Scale (BBS). PubMed
-
Mini-BESTest – breaks balance into sub-domains (anticipatory, reactive, sensory orientation, dynamic gait) for more precise guidance. PubMed
-
Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA) – assesses gait under challenges (head turns, speed changes); can still have ceiling effects in high-functioning patients. Frontiers
C. Targeted vestibular/oculomotor testing
-
Head Impulse Test, Dix-Hallpike, VOR tests, convergence, saccades, smooth pursuits
-
Computerized dynamic visual acuity, optokinetic sensitivity screens
-
Benign paroxysmal positional vertigo (BPPV) maneuvers when appropriate
D. Instrumented balance & motion analysis
-
Force-plate or Limits of Stability (LOS) testing—more sensitive to subtle postural control changes and linked to dizziness outcomes. PubMed
-
Perturbation & reactive stepping assessments—capture the quick corrections often impaired after concussion. Frontiers
E. Imaging and advanced studies (as indicated by clinicians)
-
CT/MRI for structural injury or complications
-
Diffusion Tensor Imaging (DTI) in select cases to assess white matter integrity
-
Autonomic testing, cerebral perfusion studies (specialized)
-
Comprehensive neuropsychological testing
Emergency category: If decorticate or decerebrate posturing is present, this is an immediate medical emergency; neurocritical care teams use established coma scales and imaging to guide treatment. Cleveland Clinic+1
Rehabilitation: Bringing the Systems Back Together
Multi-sensory retraining
A core goal is to help the brain reweight inputs from the vision, vestibular organs, and proprioception, so the person can balance automatically again. Reviews of balance after TBI emphasize that dizziness, unsteadiness, and imbalance are frequent and that testing and treatment should span these domains. PMC
Sample progression (always individualized):
-
Gaze stabilization (eyes on a target while moving the head)
-
Sensory orientation (standing on firm vs. foam, eyes open vs. closed)
-
Reactive control (light taps or nudges requiring quick steps)
-
Dual-task (walking while counting; gentle head turns while scanning aisles)
-
Community mobility (curbs, crowds, low-light situations)
Cervical and upper thoracic care
-
Manual therapy & adjustments (when appropriate) to restore segmental motion and normalize afferent input to the brainstem and cerebellum
-
Deep neck flexor training and scapular stabilization to correct forward-head posture
-
Breathing drills to reduce over-bracing and improve trunk control
A growing number of clinics describe integrative programs that combine these elements and report symptomatic improvements; while more high-quality trials are needed, this team-based, multimodal approach is widely recommended in practice. Northwest Florida Physicians Group+2Impact Medical Group+2
Day-to-Day Strategies to Support Posture After TBI
-
Adopt a “stacked” posture during screens: keep your ears over your shoulders, gently nod your chin, and position your ribs over your pelvis.
-
Use visual anchors in busy spaces (fix your gaze on a stable point).
-
Micro-breaks every 30–60 minutes: 3 slow breaths, shoulder rolls, gentle neck range-of-motion.
-
Walk with purpose: start on firm ground, add head turns later.
-
Hydration, protein, and omega-3-rich foods to support tissue repair and energy for rehab.
-
Establish a consistent sleep routine (consistent bedtime, low light, and screens off) to support neuroplasticity.
-
Pace activities: stop before symptoms spike; resume after symptoms settle.
-
Home safety: good lighting, remove trip hazards, supportive footwear.
When to Seek Immediate Care
-
Abnormal posturing (arms drawn in and legs rigid; or arms/legs extended and arched back)
-
Worsening headache, repeated vomiting, fainting, seizures
-
New weakness, vision loss, slurred speech
These signs can indicate severe brain damage or pressure changes and need urgent evaluation. Cleveland Clinic+1
Putting It All Together
-
Mild TBIs often leave subtle, persistent balance changes because the brain must re-integrate visual, vestibular, and body sensation inputs. This can be measured with sensitive tests and treated with targeted rehab. PMC+1
-
Severe TBIs can produce decorticate or decerebrate posturing, which is an emergency. Cleveland Clinic+1
-
Cervical and upper thoracic problems often co-occur with symptoms such as headaches and dizziness; addressing neck mechanics can improve posture and balance. PMC
-
An integrative, team-based plan—medical oversight, chiropractic care for alignment and mobility, and vestibular/sensory-motor therapies—offers a practical, patient-centered path to recovery. Northwest Florida Physicians Group+1
Final Takeaways
-
Mild TBI can lead to long-lasting balance and posture changes, even when routine tests appear normal. Sensitive balance measures and cervical evaluation are key. PMC+1
-
Severe TBI may lead to decorticate or decerebrate posturing—both are medical emergencies. Cleveland Clinic+1
-
Neck and upper thoracic mechanics can exacerbate headaches and dizziness, and impact posture; addressing these issues often supports better rehabilitation outcomes. PMC
-
An integrative plan—medical oversight, chiropractic adjustments when appropriate, vestibular and sensory-motor therapies, and lifestyle support—offers a practical path back to steady posture and confident movement. Northwest Florida Physicians Group+1
References
Cleveland Clinic. (2023). Decerebrate posturing: What it is, causes, & treatment. https://my.clevelandclinic.org/health/symptoms/24968-decerebrate-posturing Cleveland Clinic
Cleveland Clinic. (2023). Decorticate posturing: What it is, causes, & treatment. https://my.clevelandclinic.org/health/symptoms/24969-decorticate-posturing Cleveland Clinic
Mount Sinai. (n.d.). Decerebrate posture. https://www.mountsinai.org/health-library/symptoms/decerebrate-posture Mount Sinai Health System
Mount Sinai. (n.d.). Decorticate posture. https://www.mountsinai.org/health-library/symptoms/decorticate-posture Mount Sinai Health System
Sosnoff, J. J., Broglio, S. P., Shin, S., & Ferrara, M. S. (2011). Previous mild traumatic brain injury and postural-control dynamics. Journal of Athletic Training, 46(1), 85–91. https://pmc.ncbi.nlm.nih.gov/articles/PMC3017494/ PMC
Row, J., et al. (2019). Balance assessment in traumatic brain injury. Frontiers in Neurology. https://pmc.ncbi.nlm.nih.gov/articles/PMC6661911/ PMC
Brain Injury Canada. (n.d.). Mobility after brain injury. https://braininjurycanada.ca/en/effects-brain-injury/physical/mobility/ braininjurycanada.ca
Brain Injury Association of America (TBI Model Systems). (2025). Factors associated with sitting and standing balance. https://biausa.org/professionals/research/tbi-model-systems/factors-associated-with-sitting-and-standing-balance Brain Injury Association of America
Morin, M., Langevin, P., & Fait, P. (2016). Cervical spine involvement in mild traumatic brain injury: A review. Journal of Sports Medicine, Article ID 1590161. https://pmc.ncbi.nlm.nih.gov/articles/PMC4977400/ PMC
Morris, A., et al. (2020). Reactive postural responses after mild traumatic brain injury. Frontiers in Sports and Active Living. https://www.frontiersin.org/articles/10.3389/fspor.2020.574848/full Frontiers
Campbell, K. R., et al. (2023). Assessment of balance in people with mild traumatic brain injury. Gait & Posture. https://pubmed.ncbi.nlm.nih.gov/36516644/ PubMed
Cleveland Clinic. (2019). What is cerebral perfusion pressure? (educational article hosted by Dr. Jimenez) https://dralexjimenez.com/what-is-cerebral-perfusion-pressure/ El Paso, TX Doctor Of Chiropractic
Jimenez, A. (2025). Traumatic brain injury: Understanding the long-term effects. https://dralexjimenez.com/traumatic-brain-injury-understanding-the-long-term-effects/ El Paso, TX Doctor Of Chiropractic
Impact Medical Group. (2024). Can chiropractic care help with mild traumatic brain injuries? https://www.impactmedicalgroup.com/2024/06/26/can-chiropractic-care-help-with-mild-traumatic-brain-injuries/ Impact Medical Group
HML Functional Care. (2025). How chiropractic neurology supports brain healing. https://hmlfunctionalcare.com/how-chiropractic-neurology-supports-brain-healing/ HML Functional Care
Pinnacle Health Chiropractic. (2025). Six ways chiropractic care supports healing after TBI. https://www.pinnaclehealthchiro.com/blog/six-ways-chiropractic-care-supports-healing-after-tbi pinnaclehealthchiro.com
Northwest Florida Physicians Group. (2025). Using chiropractic care to treat traumatic brain injuries. https://northwestfloridaphysiciansgroup.com/using-chiropractic-care-to-treat-traumatic-brain-injuries/ Northwest Florida Physicians Group
Vida Integrated Health. (2025). Treating concussions with chiropractic care. https://thinkvida.com/blog/treating-concussions-with-chiropractic-care/ Vida Integrated Health
Jimenez, A. (LinkedIn profile). (n.d.). https://www.linkedin.com/in/dralexjimenez/ El Paso, TX Doctor Of Chiropractic
Optional further reading used in background:
-
Buckley, T. A., et al. (2016). Postural control deficits identify lingering post-concussion impairments. https://pmc.ncbi.nlm.nih.gov/articles/PMC6191989/ PMC
Post Disclaimer
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Traumatic Brain Injury and Posture: Signs and Solutions" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine; wellness; contributing etiological viscerosomatic disturbances within clinical presentations; associated somato-visceral reflex clinical dynamics; subluxation complexes; sensitive health issues; and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and licensure jurisdiction. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that directly or indirectly relate to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
New Mexico CNP License#: 90560, Verified
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
| Yes | 363LF0000X - Nurse Practitioner - Family | NM |
90560 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
📆 Schedule Appointment: Schedule 24/7 (Click Here)