


Hip pain is a well-known health issue which can be caused by a wide array of problems, however, the site of the patient’s hip pain can provide valuable information regarding the underlying cause of this common health issue. Pain on the inside of the hip or groin can be due to problems within the hip joint itself while pain on the outside of the hip, upper thigh and outer buttocks may be due to problems with the ligaments, tendons
Table of Contents
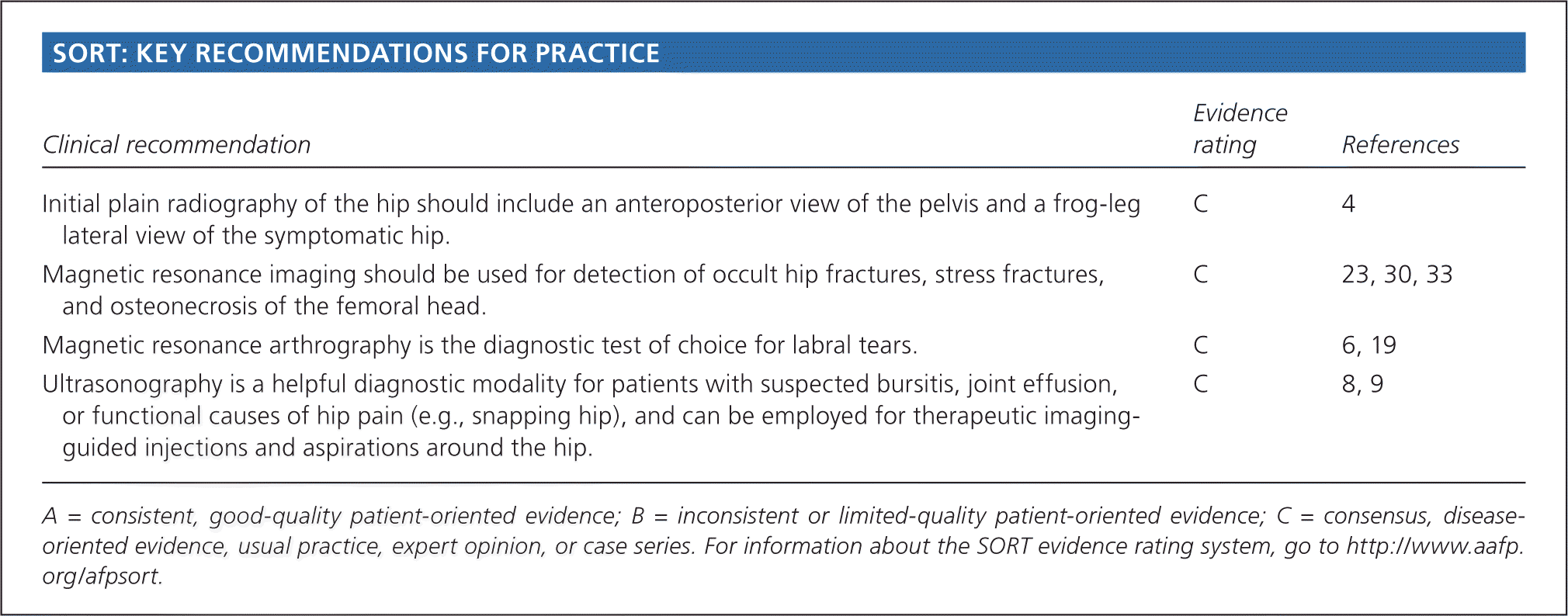
Abstract
Hip pain is a common and disabling condition that affects patients of all ages. The differential diagnosis of hip pain is broad, presenting a diagnostic challenge. Patients often express that their hip pain is localized to one of three anatomic regions: the anterior hip and groin, the posterior hip and buttock, or the lateral hip. Anterior hip and groin pain is commonly associated with intra-articular pathology, such as osteoarthritis and hip labral tears. Posterior hip pain is associated with piriformis syndrome, sacroiliac joint dysfunction, lumbar radiculopathy, and less commonly ischiofemoral impingement and vascular claudication. Lateral hip pain occurs with greater trochanteric pain syndrome. Clinical examination tests, although helpful, are not highly sensitive or specific for most diagnoses; however, a rational approach to the hip examination can be used. Radiography should be performed if acute fracture, dislocations, or stress fractures are suspected. Initial plain radiography of the hip should include an anteroposterior view of the pelvis and frog-leg lateral view of the symptomatic hip. Magnetic resonance imaging should be performed if the history and plain radiograph results are not diagnostic. Magnetic resonance imaging is valuable for the detection of occult traumatic fractures, stress fractures, and osteonecrosis of the femoral head. Magnetic resonance arthrography is the diagnostic test of choice for labral tears.
Introduction
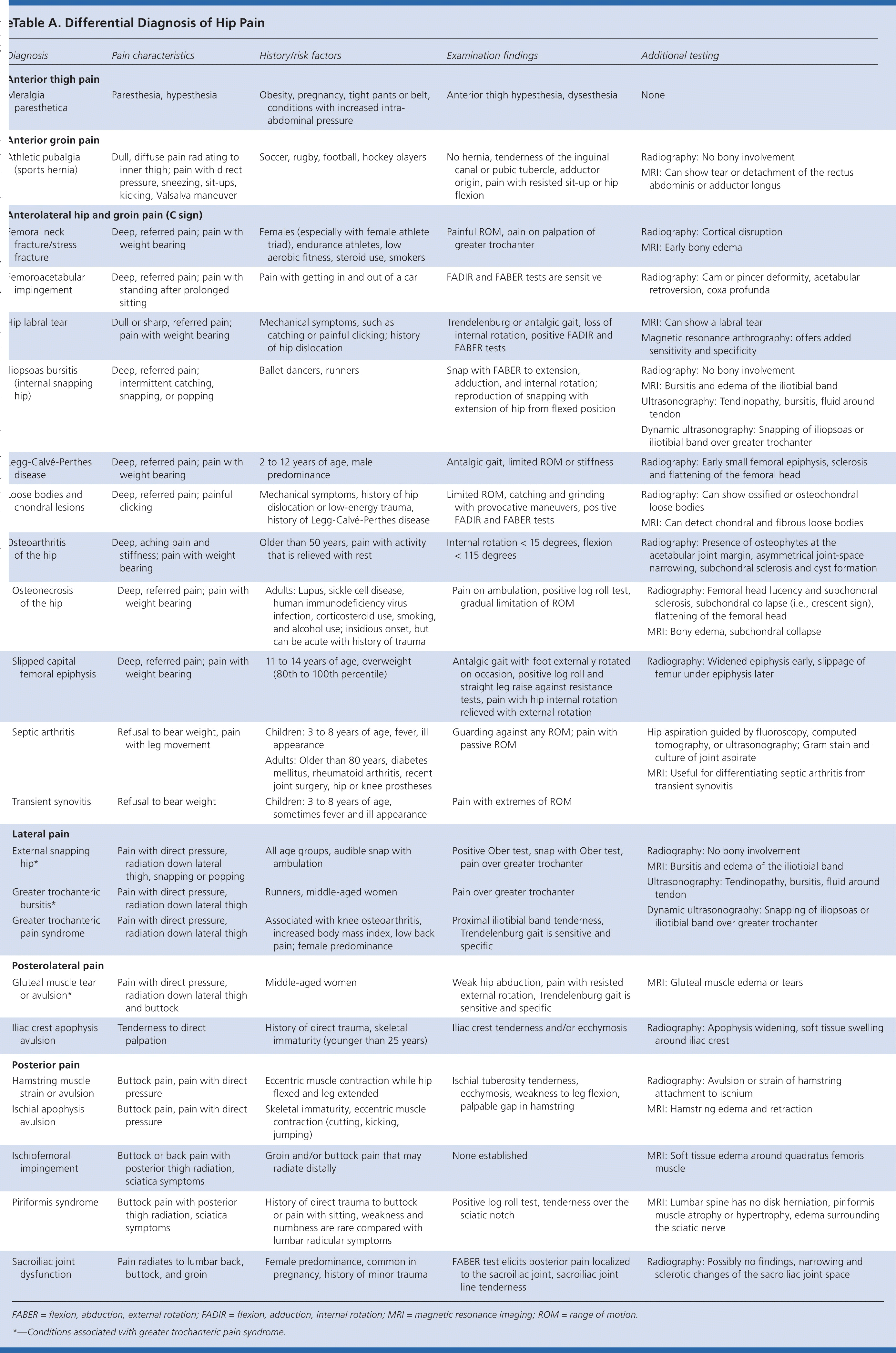
Hip pain is a common presentation in primary care and can affect patients of all ages. In one study, 14.3% of adults 60 years and older reported significant hip pain on most days over the previous six weeks.1 Hip pain often presents a diagnostic and therapeutic challenge. The differential diagnosis of hip pain (eTable A) is broad, including both intra-articular and extra-articular pathology, and varies by age. A history and physical examination are essential to accurately diagnose the cause of hip pain.
Anatomy
The hip joint is a ball-and-socket synovial joint designed to allow multiaxial motion while transferring loads between the upper and lower body. The acetabular rim is lined by fibrocartilage (labrum), which adds depth and stability to the
The hip joint’s wide range of motion is second only to that of the glenohumeral joint and is enabled by the large number of muscle groups that surround the hip. The flexor muscles include the iliopsoas, rectus femoris, pectineus, and sartorius muscles. The gluteus maximus and hamstring muscle groups allow for hip extension. Smaller muscles, such as gluteus medius and minimus, piriformis, obturator externus and internus, and quadratus femoris muscles, insert around the greater trochanter, allowing for abduction, adduction, and internal and external rotation.
In persons who are skeletally immature, there are several growth centers of the pelvis and femur where injuries can occur. Potential sites of apophyseal injury in the hip region include the ischium, anterior superior iliac spine, anterior inferior iliac spine, iliac crest, lesser trochanter, and greater trochanter. The apophysis of the superior iliac spine matures last and is susceptible to injury up to 25 years of age.2

The hip joint is one of the larger joints found in the human body and it serves in locomotion as the thigh moves forward and backward. The hip joint also rotates when sitting and with changes of direction while walking. A variety of complex structures surround the hip joint. When an injury or condition affects these, it can ultimately lead to hip pain.
Dr. Alex Jimenez D.C., C.C.S.T.
Evaluation of Hip Pain
History
Age alone can narrow the differential diagnosis of hip pain. In prepubescent and adolescent patients, congenital malformations of the
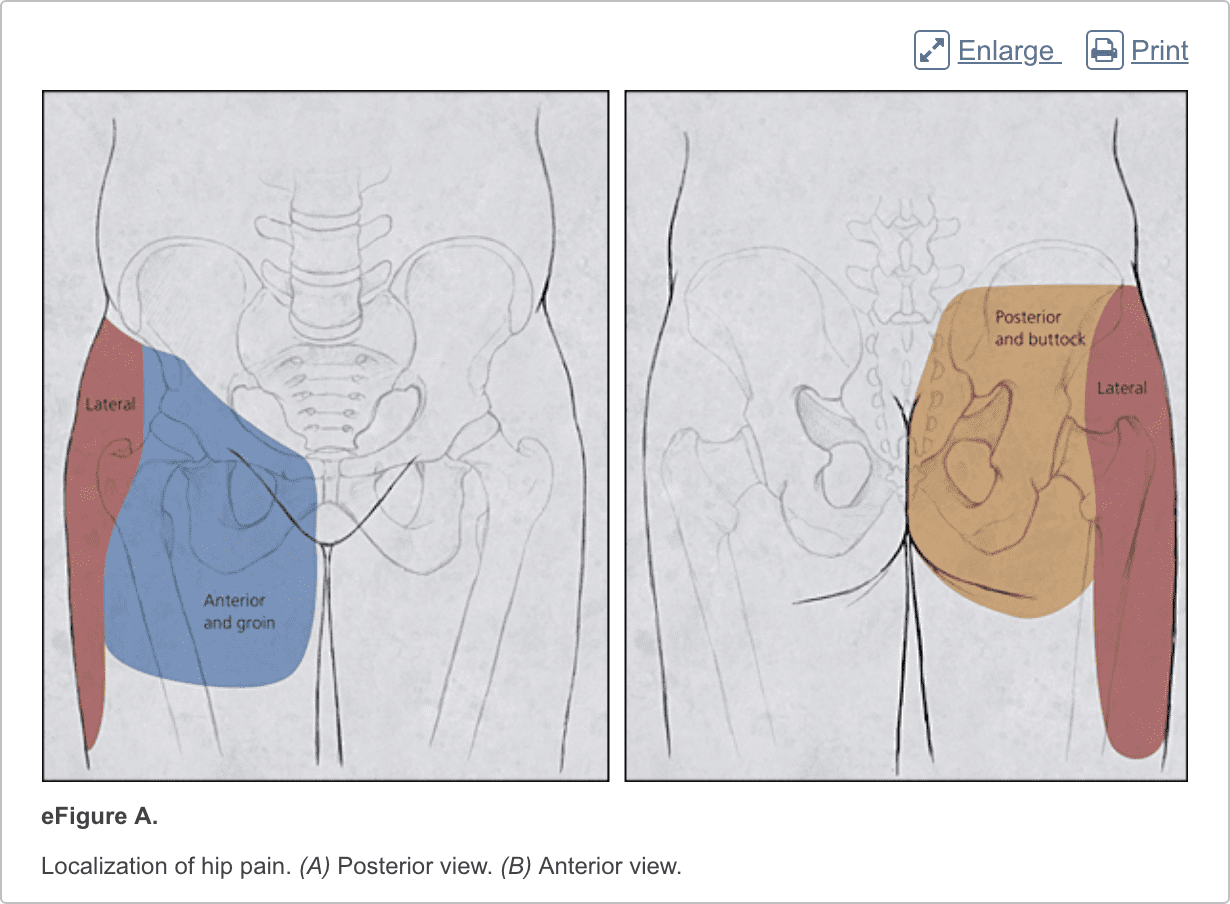
Patients with hip pain should be asked about antecedent trauma or inciting activity, factors that increase or decrease the pain, mechanism of injury, and time of onset. Questions related to hip function, such as the ease of getting in and out of a car, putting on shoes, running, walking, and going up and down stairs, can be helpful.3 Location of the pain is informative because hip pain often localizes to one of three basic anatomic regions: the anterior hip and groin, posterior hip and buttock, and lateral hip (eFigure A).
Physical Examination
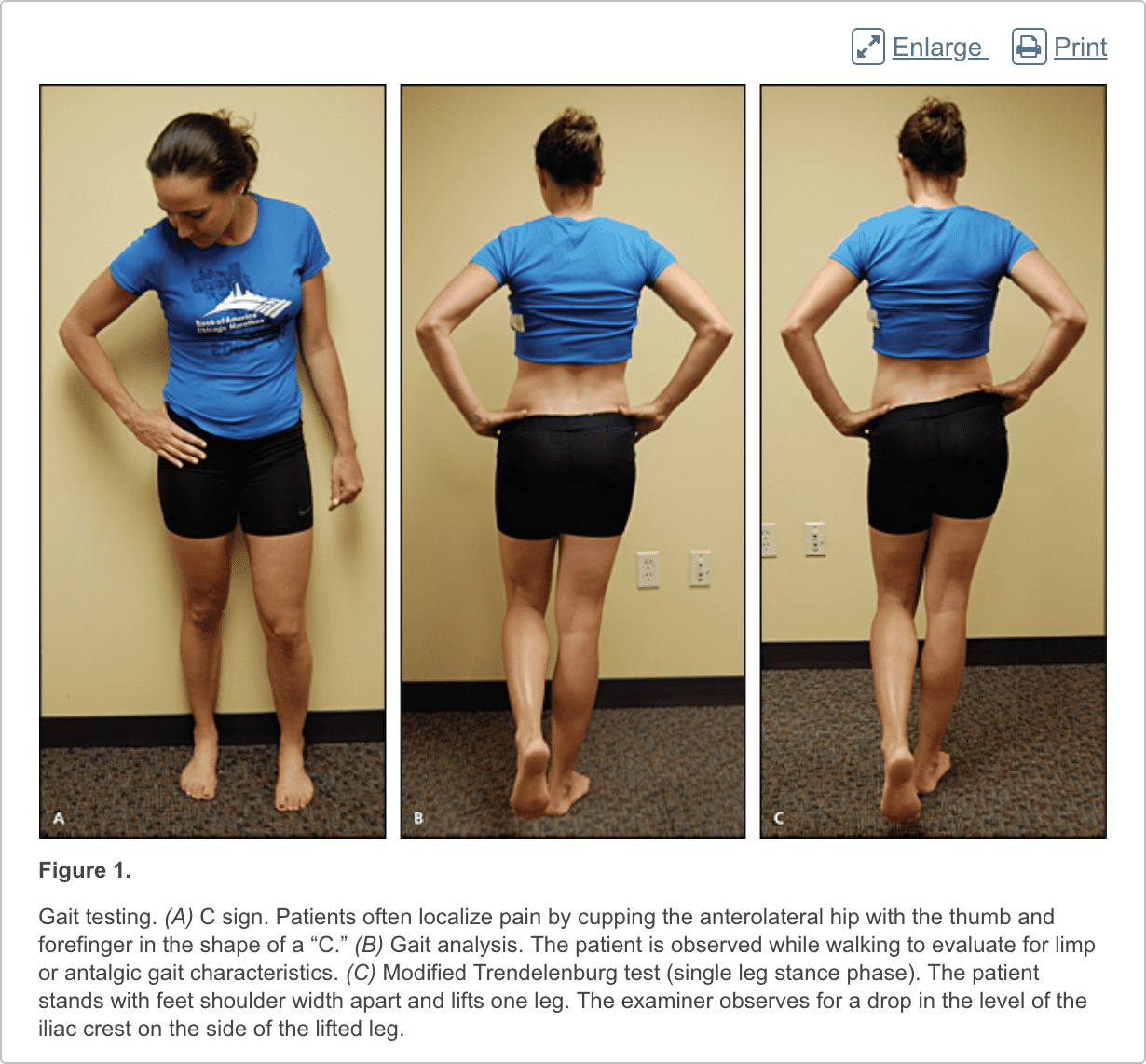
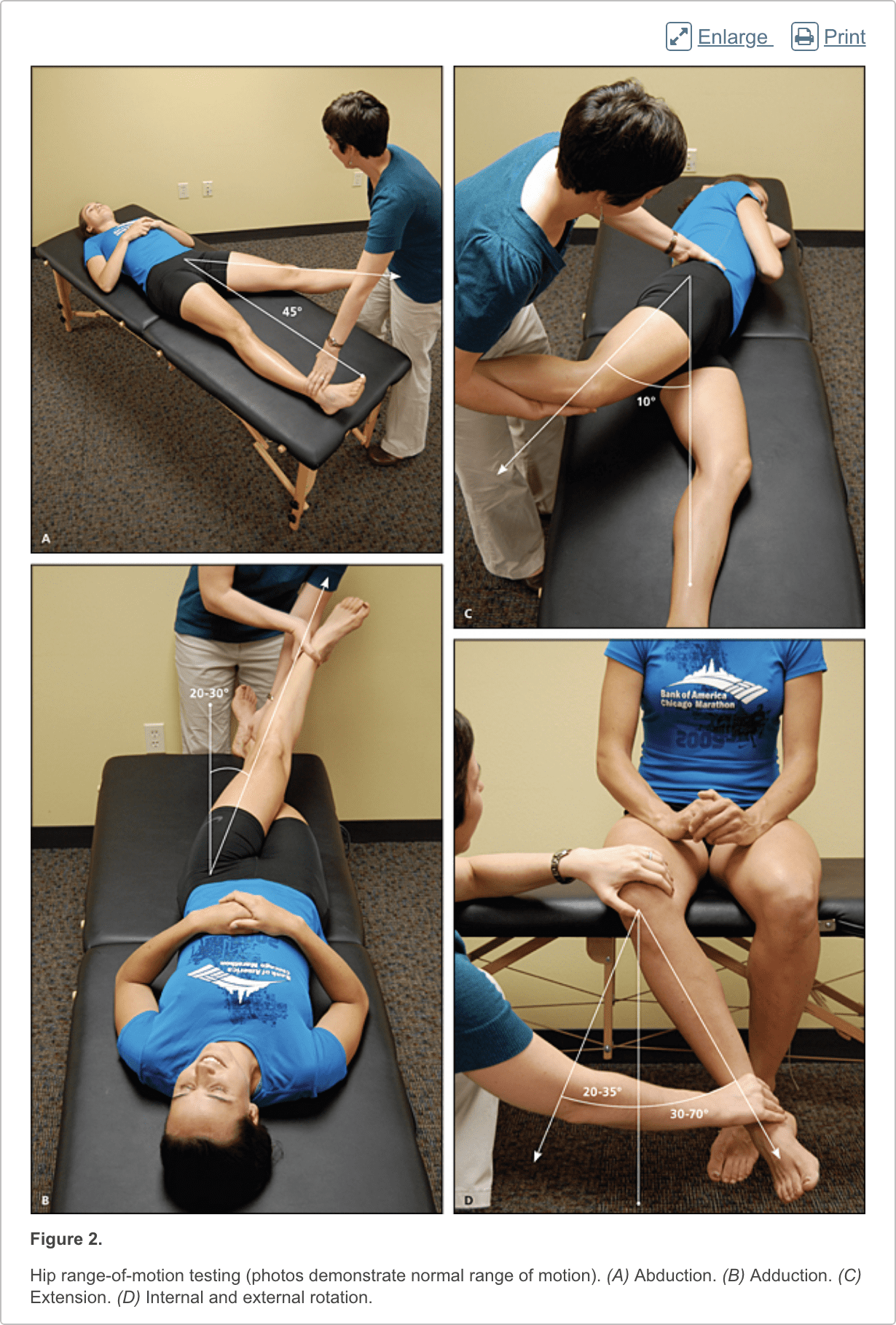
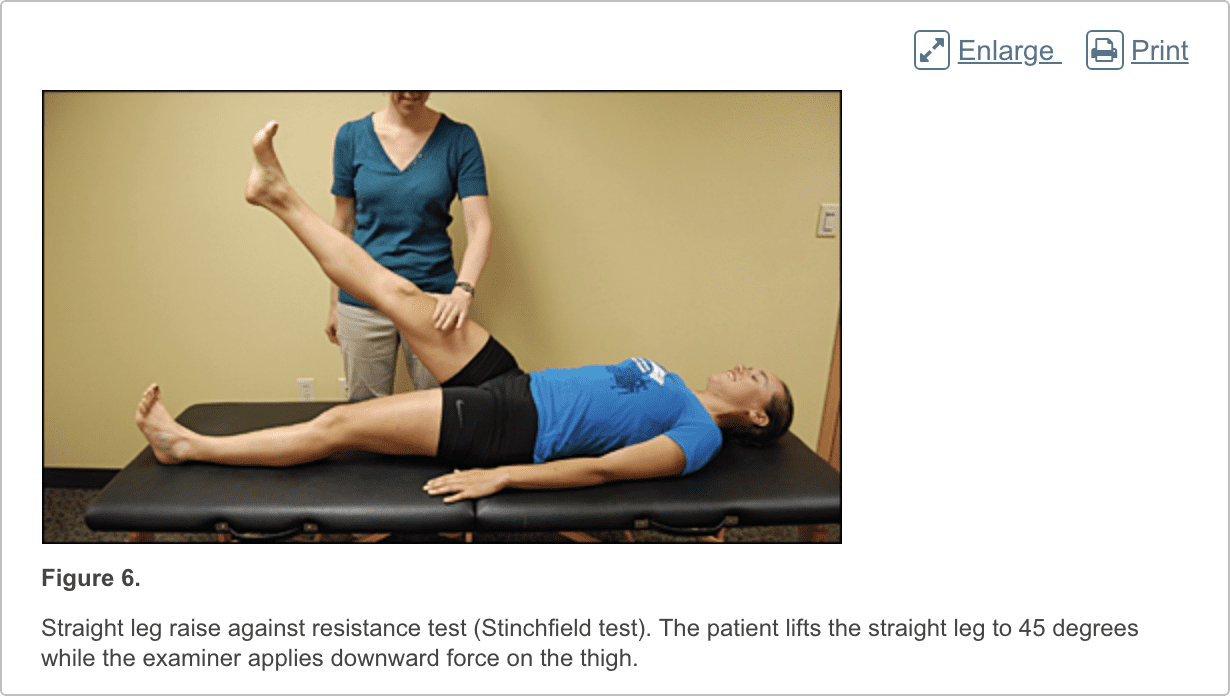
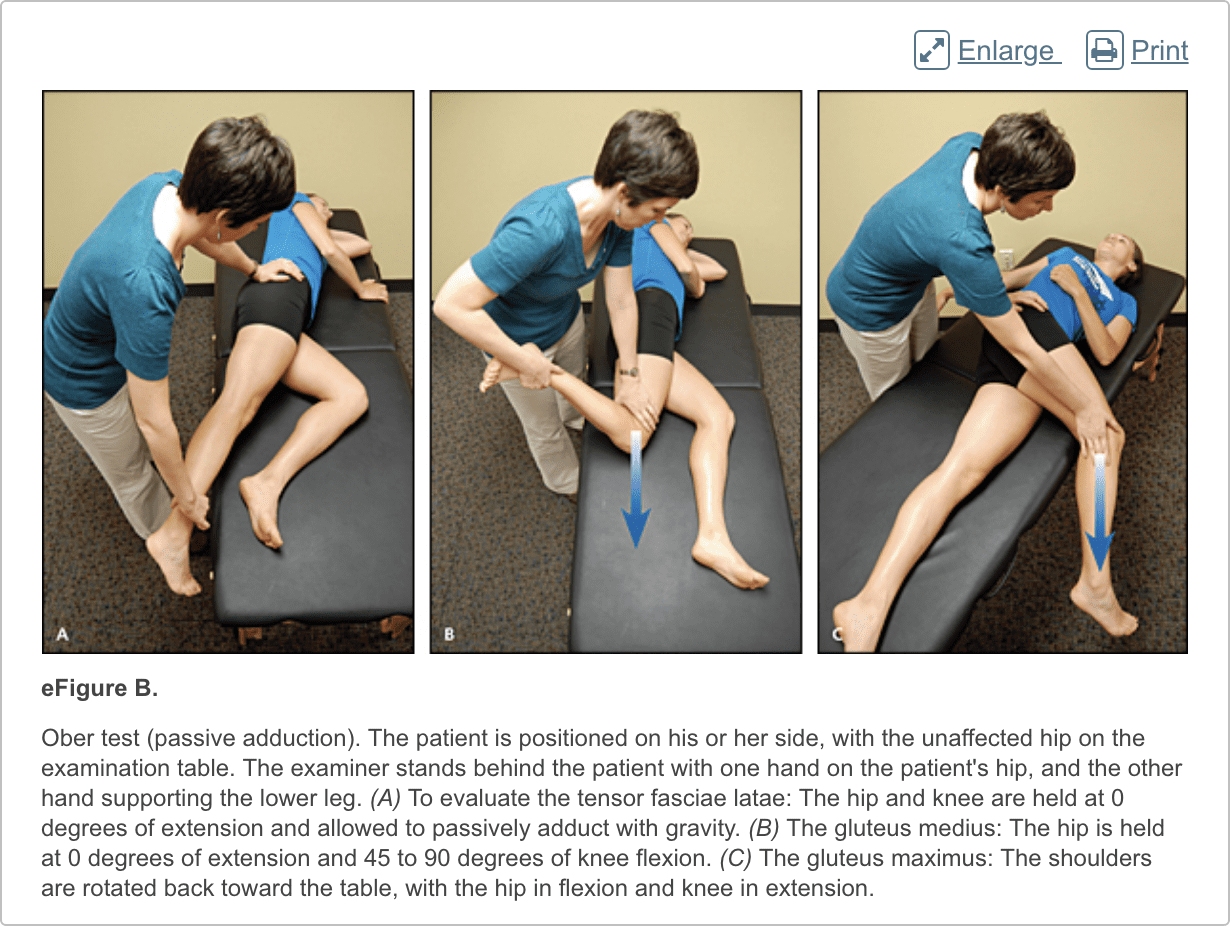
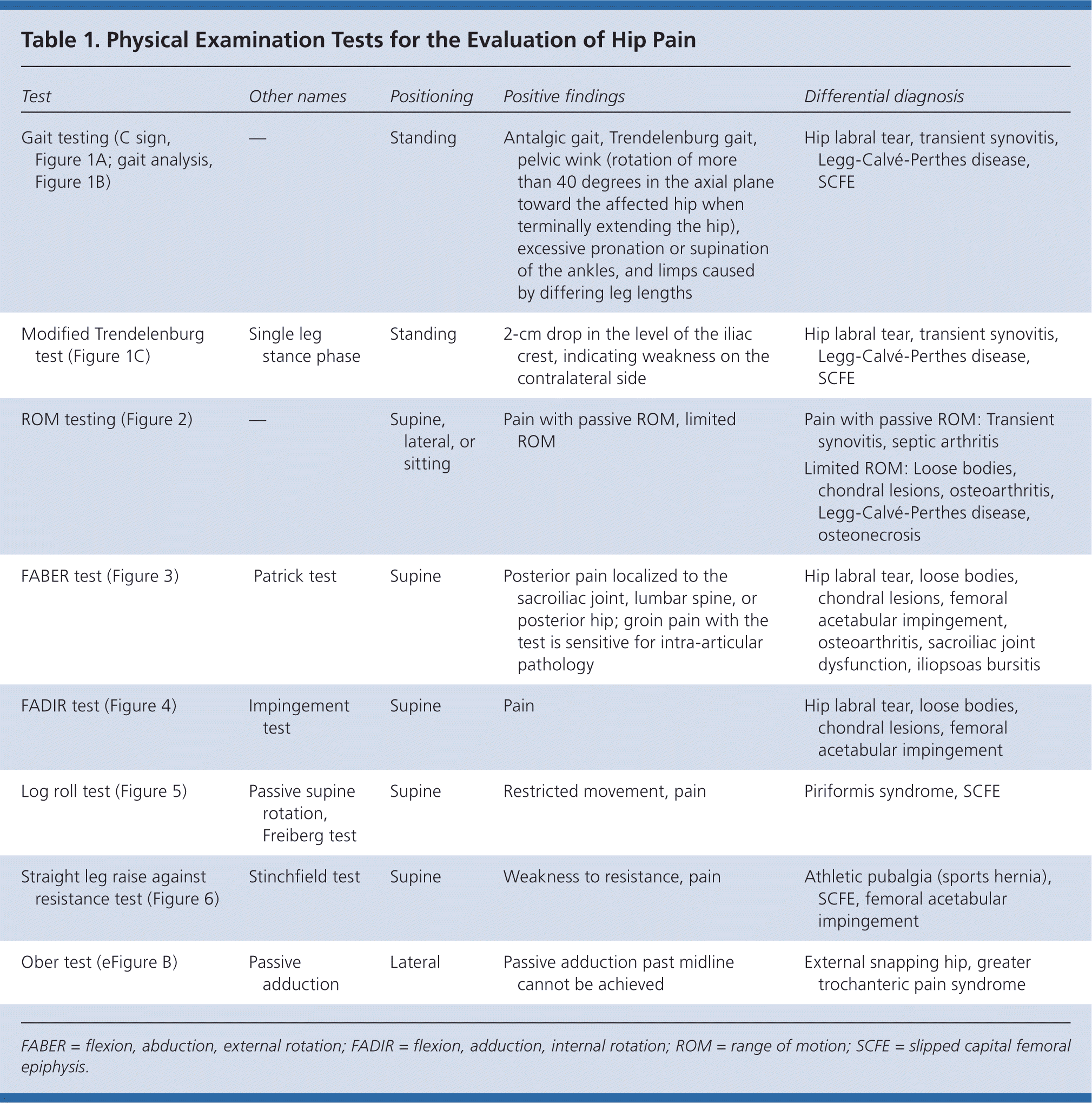
The hip examination should evaluate the hip, back, abdomen, and vascular and neurologic systems. It should start with a gait analysis and stance assessment (Figure 1), followed by evaluation of the patient in seated, supine, lateral, and prone positions (Figures 2 through 6, and eFigure B). Physical examination tests for the evaluation of hip pain are summarized in Table 1.
Imaging
Radiography. Radiography of the hip should be performed if there is any suspicion of acute fracture, dislocation, or stress fracture. Initial plain radiography of the hip should include an anteroposterior view of the pelvis and a frog-leg lateral view of the symptomatic hip.4
Magnetic Resonance Imaging and Arthrography. Conventional magnetic resonance imaging (MRI) of the hip can detect many soft tissue abnormalities, and is the preferred imaging modality if plain radiography does not identify specific pathology in a patient with persistent pain.5 Conventional MRI has a sensitivity of 30% and an accuracy of 36% for diagnosing hip labral tears, whereas magnetic resonance arthrography provides added sensitivity of 90% and accuracy of 91% for the detection of labral tears.6,7
Ultrasonography. Ultrasonography is a useful technique for evaluating individual tendons, confirming suspected bursitis, and identifying joint effusions and functional causes of hip pain.8 Ultrasonography is especially useful for safely and accurately performing imaging-guided injections and aspirations around the hip.9 It is ideal for an experienced ultrasonographer to perform the diagnostic study; however, emerging evidence suggests that less experienced clinicians with appropriate training can make diagnoses with reliability similar to that of an experienced musculoskeletal ultrasonographer.10,11
These are numerous causes for hip pain. Although some hip pain may only be temporary, other forms of hip pain can become chronic if left untreated for an extended period of time. Several common causes of hip pain include, arthritis, fracture, sprain, avascular necrosis, Gaucher’s disease, sciatica, muscle strain, iliotibial band syndrome or IT band syndrome and hematoma, among others described below.
Dr. Alex Jimenez D.C., C.C.S.T.
Differential Diagnosis of Anterior Hip Pain
Anterior hip or groin pain suggests involvement of the hip joint itself. Patients often localize pain by cupping the anterolateral hip with the thumb and forefinger in the shape of a “C.” This is known as the C sign (Figure 1A).
Osteoarthritis
Osteoarthritis is the most likely diagnosis in older adults with limited motion and gradual onset of symptoms. Patients have a constant, deep, aching pain and stiffness that are worse with prolonged standing and weight bearing. Examination reveals decreased range of motion, and extremes of hip motion often cause pain. Plain radiographs demonstrate the presence of asymmetrical joint-space narrowing, osteophytosis, and subchondral sclerosis and cyst formation.12
Femoroacetabular Impingement
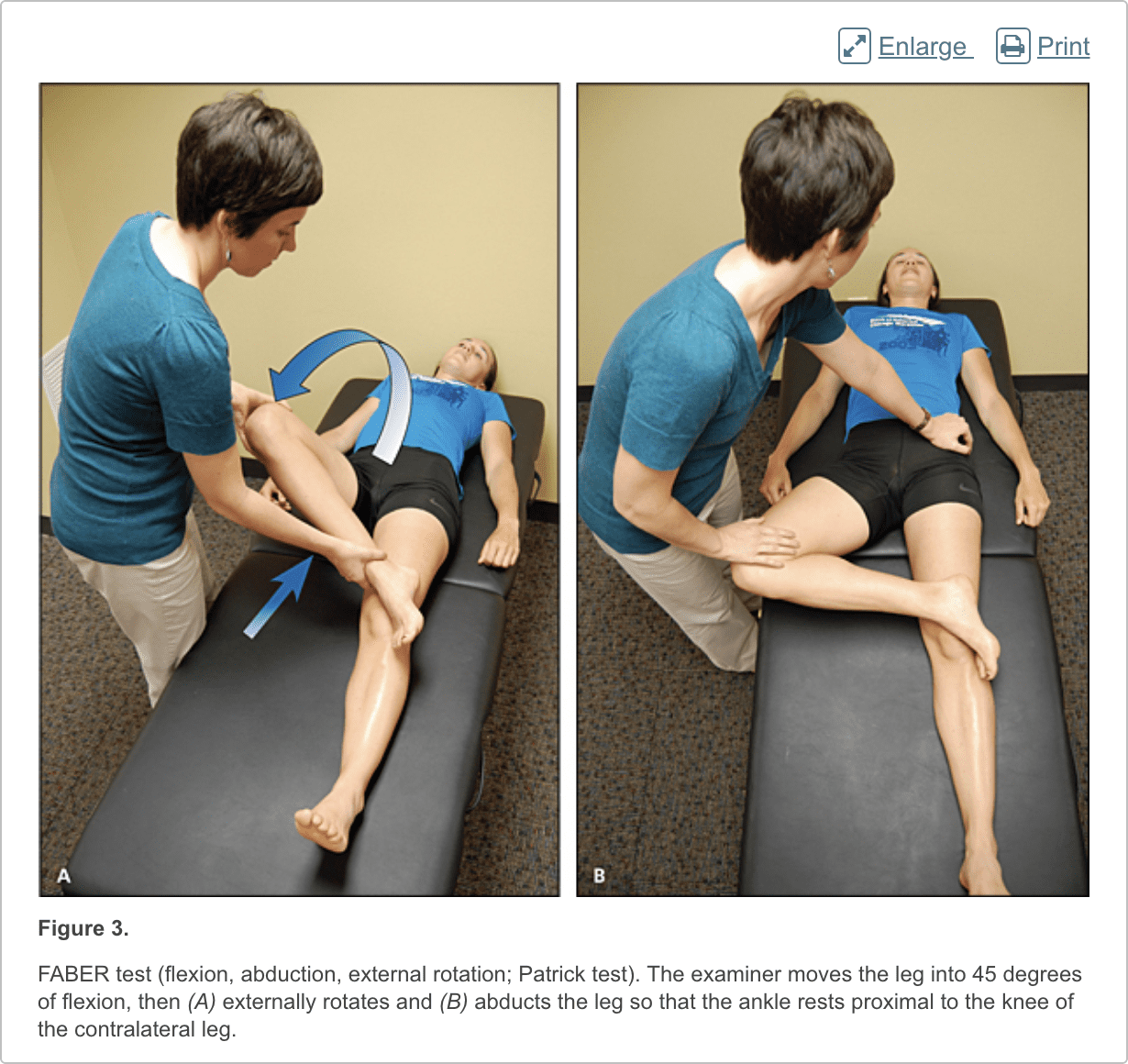
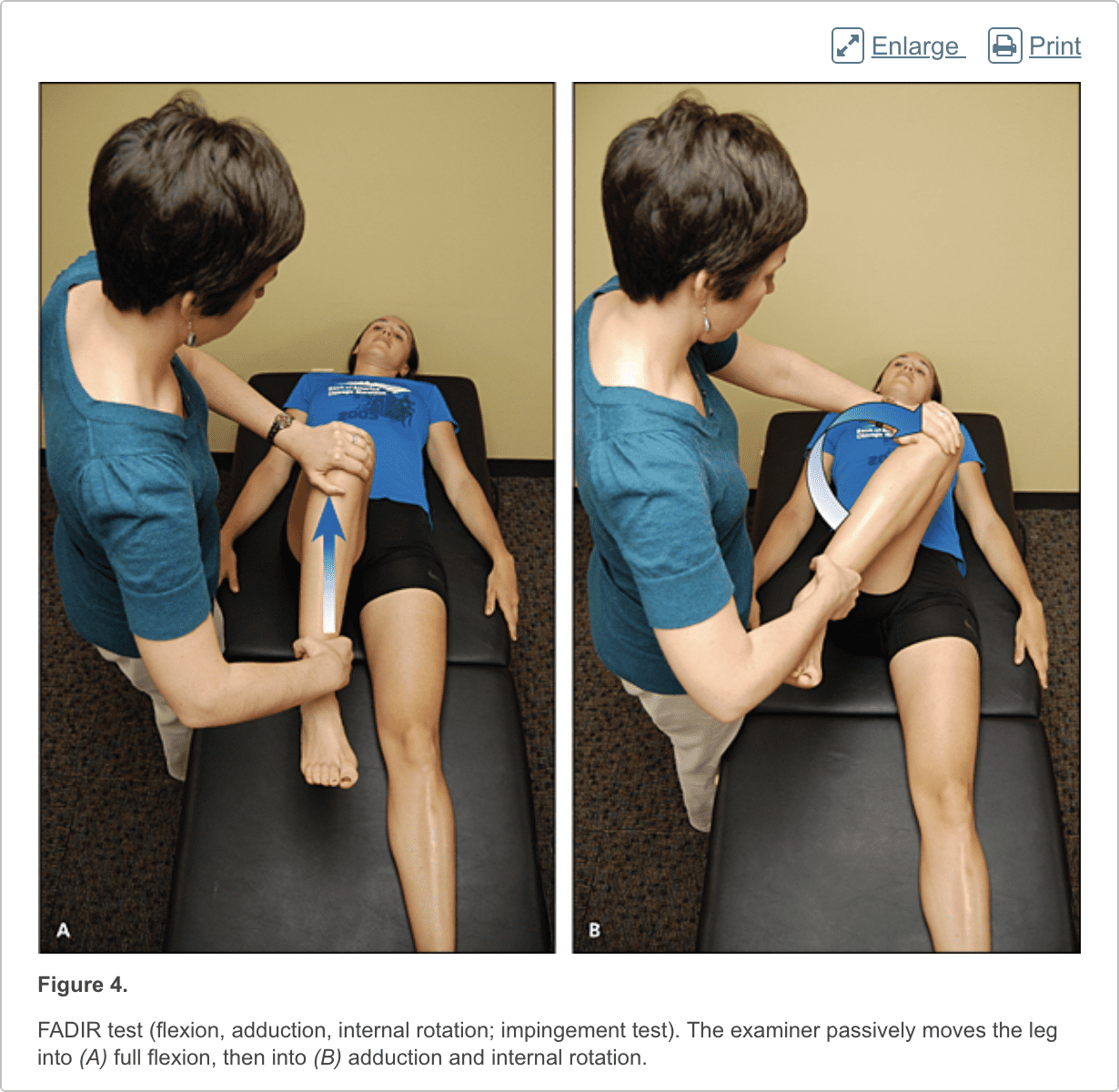
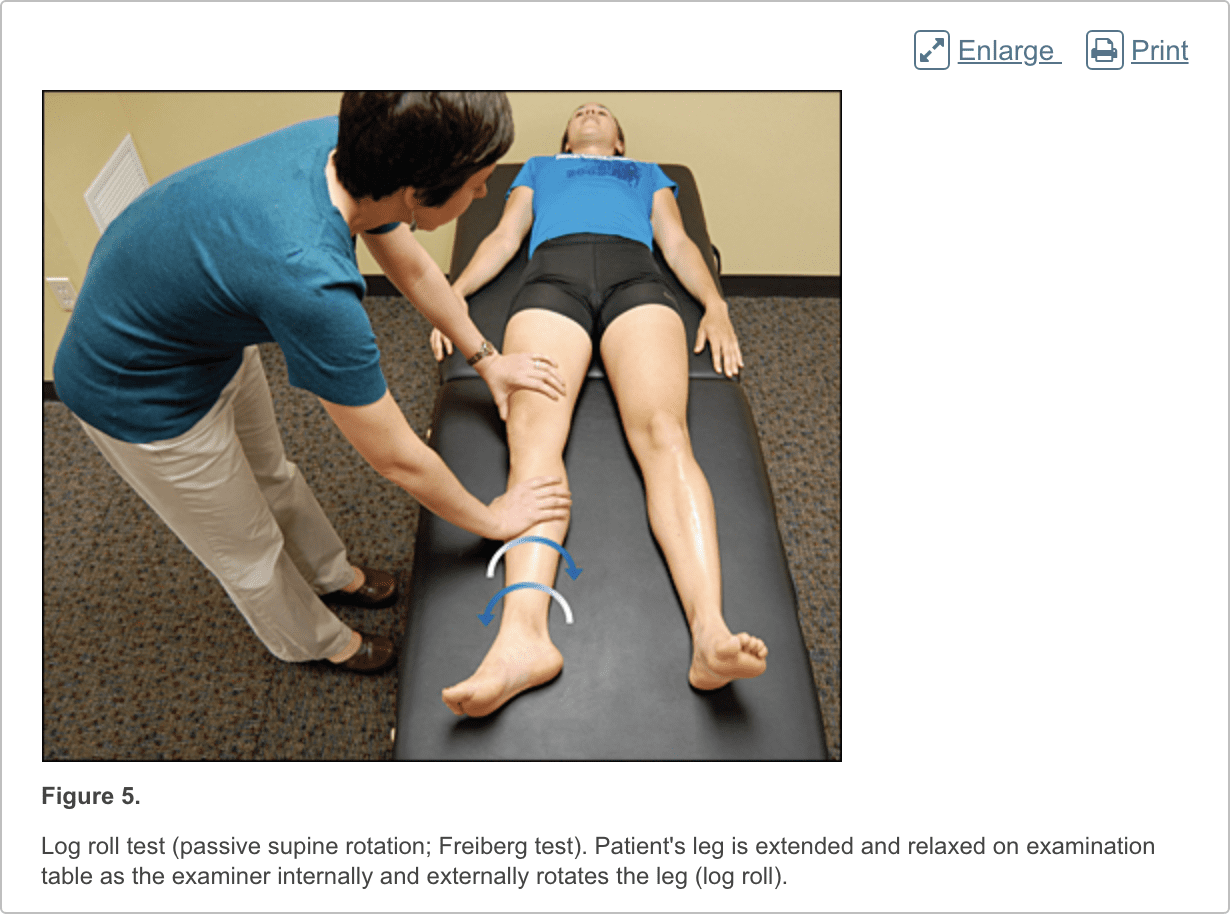
Patients with femoroacetabular impingement are often young and physically active. They describe insidious onset of pain that is worse with sitting, rising from a seat, getting in or out of a car, or leaning forward.13 The pain is located primarily in the groin with occasional radiation to the lateral hip and anterior thigh.14 The FABER test (flexion, abduction, external rotation; Figure 3) has a sensitivity of 96% to 99%. The FADIR test (flexion, adduction, internal rotation; Figure 4), log roll test (Figure 5), and straight leg raise against resistance test (Figure 6) are also effective, with sensitivities of 88%, 56%, and 30%, respectively.14,15 In addition to the anteroposterior and lateral radiograph views, a Dunn view should be obtained to help detect subtle lesions.16
Hip Labral Tear
Hip labral tears cause dull or sharp groin pain, and one-half of patients with a labral tear have pain that radiates to the lateral hip, anterior thigh, and buttock. The pain usually has an insidious onset, but occasionally begins acutely after a traumatic event. About one-half of patients with this injury also have mechanical symptoms, such as catching or painful clicking with activity.17 The FADIR and FABER tests are effective for detecting intra-articular pathology (the sensitivity is 96% to 75% for the FADIR test and is 88% for the FABER test), although neither test has high specificity.14,15,18 Magnetic resonance arthrography is considered the diagnostic test of choice for labral tears.6,19 However, if a labral tear is not suspected, other less invasive imaging modalities, such as plain radiography and conventional MRI, should be used first to rule out other causes of hip and groin pain.
Iliopsoas Bursitis (Internal Snapping Hip)
Patients with this condition have anterior hip pain when extending the hip from a flexed position, often associated with intermittent catching, snapping, or popping of the hip.20 Dynamic real-time ultrasonography is particularly useful in evaluating the various forms of snapping hip.8
Occult or Stress Fracture
Occult or stress fracture of the hip should be considered if trauma or repetitive weight-bearing exercise is involved, even if plain radiograph results are negative.21 Clinically, these injuries cause anterior hip or groin pain that is worse with activity.21 Pain may be present with extremes of motion, active straight leg raise, the log roll test, or hopping.22 MRI is useful for the detection of occult traumatic fractures and stress fractures not seen on plain radiographs.23
Transient Synovitis and Septic Arthritis
Acute onset of atraumatic anterior hip pain that results in impaired weight bearing should raise suspicion for transient synovitis and septic arthritis. Risk factors for septic arthritis in adults include age older than 80 years, diabetes mellitus, rheumatoid arthritis, recent joint surgery, and hip or knee prostheses.24 Fever, complete blood count, erythrocyte sedimentation rate, and C-reactive protein level should be used to evaluate the risk of septic arthritis.25,26 MRI is useful for differentiating septic arthritis from transient synovitis.27,28 However, hip aspiration using guided imaging such as fluoroscopy, computed tomography, or ultrasonography is recommended if a septic joint is suspected.29
Osteonecrosis
Legg-Calvé-Perthes disease is an idiopathic osteonecrosis of the femoral head in children two to 12 years of age, with a male-to-female ratio of 4:1.4 In adults, risk factors for osteonecrosis include systemic lupus erythematosus, sickle cell disease, human immunodeficiency virus infection, smoking, alcoholism, and corticosteroid use.30,31 Pain is the presenting symptom and is usually insidious. Range of motion is initially preserved but can become limited and painful as the disease progresses.32 MRI is valuable in the diagnosis and prognostication of osteonecrosis of the femoral head.30,33
Differential Diagnosis of Posterior Hip and Buttock Pain
Piriformis Syndrome and Ischiofemoral Impingement
Piriformis syndrome causes buttock pain that is aggravated by sitting or walking, with or without ipsilateral radiation down the posterior thigh from sciatic nerve compression.34,35 Pain with the log roll test is the most sensitive test, but tenderness with palpation of the sciatic notch can help with the diagnosis.35
Ischiofemoral impingement is a less well-understood condition that can lead to nonspecific buttock pain with radiation to the posterior thigh.36,37 This condition is thought to be a result of impingement of the quadratus femoris muscle between the lesser trochanter and the ischium.
Unlike sciatica from disc herniation, piriformis syndrome and ischiofemoral impingement are exacerbated by active external hip rotation. MRI is useful for diagnosing these conditions.38
Other
Other causes of posterior hip pain include sacroiliac joint dysfunction,39 lumbar radiculopathy,40 and vascular claudication.41 The presence of a limp, groin pain, and limited internal rotation of the hip is more predictive of hip disorders than disorders originating from the low back.42
Differential Diagnosis of Lateral Hip Pain
Greater Trochanteric Pain Syndrome
Lateral hip pain affects 10% to 25% of the general population.43 Greater trochanteric pain syndrome refers to pain over the greater trochanter. Several disorders of the lateral hip can lead to this type of pain, including iliotibial band thickening, bursitis, and tears of the gluteus medius and minimus muscle attachment.43–45 Patients may have mild morning stiffness and may be unable to sleep on the affected side. Gluteus minimus and medius injuries present with pain in the posterior lateral aspect of the hip as a result of partial or full-thickness tearing at the gluteal insertion. Most patients have an atraumatic, insidious onset of symptoms from repetitive use.43,45,46
In conclusion, hip pain is a common complaint which may occur due to a wide variety of health issues. Moreover, the precise location of the patient’s hip pain can provide valuable information to healthcare professionals regarding the underlying cause of the problem. The purpose of the article above was to demonstrate and discuss the evaluation of the patient with hip pain. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Data Sources: We searched articles on hip pathology in American Family Physician, along with their references. We also searched the Agency for Healthcare Research and Quality Evidence Reports, Clinical Evidence, Institute for Clinical Systems Improvement, the U.S. Preventive Services Task Force guidelines, the National Guideline Clearinghouse, and UpToDate. We performed a PubMed search using the keywords greater trochanteric pain syndrome, hip pain physical examination, imaging femoral hip stress fractures, imaging hip labral tear, imaging osteomyelitis,
Author Information: Aafp.org
1. Christmas C, Crespo CJ, Franckowiak SC, et al. How common is hip pain among older adults? Results from the Third National Health and Nutrition Examination Survey. J Fam Pract. 2002;51(4):345–348.
2. Rossi F, Dragoni S. Acute avulsion fractures of the pelvis in adolescent competitive athletes. Skeletal Radiol. 2001;30(3):127–131.
3. Martin HD, Shears SA, Palmer IJ. Evaluation of the hip. Sports Med Arthrosc. 2010;18(2):63–75.
4. Gough-Palmer A, McHugh K. Investigating hip pain in a well child. BMJ. 2007;334(7605):1216–1217.
5. Bencardino JT, Palmer WE. Imaging of hip disorders in athletes. Radiol Clin North Am. 2002;40(2):267–287.
6. Czerny C, Hofmann S, Neuhold A, et al. Lesions of the acetabular labrum: accuracy of MR imaging and MR arthrography in detection and staging. Radiology. 1996;200(1):225–230.
7. Czerny C, Hofmann S, Urban M, et al. MR arthrography of the adult acetabular capsular-labral complex. AJR Am J Roentgenol. 1999;173(2):345–349.
8. Deslandes M, Guillin R, Cardinal E, et al. The snapping iliopsoas tendon: new mechanisms using dynamic sonography. AJR Am J Roentgenol. 2008;190(3):576–581.
9. Blankenbaker DG, De Smet AA. Hip injuries in athletes. Radiol Clin North Am. 2010;48(6):1155–1178.
10. Balint PV, Sturrock RD. Intraobserver repeatability and interobserver reproducibility in musculoskeletal ultrasound imaging measurements. Clin Exp Rheumatol. 2001;19(1):89–92.
11. Ramwadhdoebe S, Sakkers RJ, Uiterwaal CS, et al. Evaluation of a training program for general ultrasound screening for developmental dysplasia of the hip in preventive child health care. Pediatr Radiol. 2010;40(10):1634–1639.
12. Altman R, Alarcón G, Appelrouth D, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991;34(5):505–514.
13. Banerjee P, McLean CR. Femoroacetabular impingement. Curr Rev Musculoskelet Med. 2011;4(1):23–32.
14. Clohisy JC, Knaus ER, Hunt DM, et al. Clinical presentation of patients with symptomatic anterior hip impingement. Clin Orthop Relat Res. 2009;467(3):638–644.
15. Ito K, Leunig M, Ganz R. Histopathologic features of the acetabular labrum in femoroacetabular impingement. Clin Orthop Relat Res. 2004;(429):262–271.
16. Beall DP, Sweet CF, Martin HD, et al. Imaging findings of femoroacetabular impingement syndrome. Skeletal Radiol. 2005;34(11):691–701.
17. Burnett RS, Della Rocca GJ, Prather H, et al. Clinical presentation of patients with tears of the acetabular labrum. J Bone Joint Surg Am. 2006;88(7):1448–1457.
18. Leunig M, Werlen S, Ungersböck A, et al. Evaluation of the acetabular labrum by MR arthrography [published correction appears in J Bone Joint Surg Br. 1997;79(4):693]. J Bone Joint Surg Br. 1997;79(2):230–234.
19. Groh MM, Herrera J. A comprehensive review of hip labral tears. Curr Rev Musculoskelet Med. 2009;2(2):105–117.
20. Blankenbaker DG, De Smet AA, Keene JS. Sonography of the iliopsoas tendon and injection of the iliopsoas bursa for diagnosis and management of the painful snapping hip. Skeletal Radiol. 2006;35(8):565–571.
21. Egol KA, Koval KJ, Kummer F, et al. Stress fractures of the femoral neck. Clin Orthop Relat Res. 1998;(348):72–78.
22. Fullerton LR Jr, Snowdy HA. Femoral neck stress fractures. Am J Sports Med. 1988;16(4):365–377.
23. Newberg AH, Newman JS. Imaging the painful hip. Clin Orthop Relat Res. 2003;(406):19–28.
24. Margaretten ME, Kohlwes J, Moore D, et al. Does this adult patient have septic arthritis? JAMA. 2007;297(13):1478–1488.
25. Eich GF, Superti-Furga A, Umbricht FS, et al. The painful hip: evaluation of criteria for clinical decision-making. Eur J Pediatr. 1999;158(11):923–928.
26. Kocher MS, Zurakowski D, Kasser JR. Differentiating between septic arthritis and transient synovitis of the hip in children. J Bone Joint Surg Am. 1999;81(12):1662–1670.
27. Learch TJ, Farooki S. Magnetic resonance imaging of septic arthritis. Clin Imaging. 2000;24(4):236–242.
28. Lee SK, Suh KJ, Kim YW, et al. Septic arthritis versus transient synovitis at MR imaging. Radiology. 1999;211(2):459–465.
29. Leopold SS, Battista V, Oliverio JA. Safety and efficacy of intraarticular hip injection using anatomic landmarks. Clin Orthop Relat Res. 2001; (391):192–197.
30. Mitchell DG, Rao VM, Dalinka MK, et al. Femoral head avascular necrosis: correlation of MR imaging, radiographic staging, radionuclide imaging, and clinical findings. Radiology. 1987;162(3):709–715.
31. Mont MA, Zywiel MG, Marker DR, et al. The natural history of untreated asymptomatic osteonecrosis of the femoral head. J Bone Joint Surg Am. 2010;92(12):2165–2170.
32. Assouline-Dayan Y, Chang C, Greenspan A, et al. Pathogenesis and natural history of osteonecrosis. Semin Arthritis Rheum. 2002;32(2):94–124.
33. Totty WG, Murphy WA, Ganz WI, et al. Magnetic resonance imaging of the normal and ischemic femoral head. AJR Am J Roentgenol. 1984;143(6):1273–1280.
34. Kirschner JS, Foye PM, Cole JL. Piriformis syndrome, diagnosis and treatment. Muscle Nerve. 2009;40(1):10–18.
35. Hopayian K, Song F, Riera R, et al. The clinical features of the piriformis syndrome. Eur Spine J. 2010;19(12):2095–2109.
36. Torriani M, Souto SC, Thomas BJ, et al. Ischiofemoral impingement syndrome. AJR Am J Roentgenol. 2009;193(1):186–190.
37. Ali AM, Whitwell D, Ostlere SJ. Case report: imaging and surgical treatment of a snapping hip due to ischiofemoral impingement. Skeletal Radiol. 2011;40(5):653–656.
38. Lee EY, Margherita AJ, Gierada DS, et al. MRI of piriformis syndrome. AJR Am J Roentgenol. 2004;183(1):63–64.
39. Slipman CW, Jackson HB, Lipetz JS, et al. Sacroiliac joint pain referral zones. Arch Phys Med Rehabil. 2000;81(3):334–338.
40. Moore KL, Dalley AF, Agur AM. Clinically Oriented Anatomy. 6th ed. Philadelphia, Pa.: Lippincott Williams & Wilkins; 2010.
41. Adlakha S, Burket M, Cooper C. Percutaneous intervention for chronic total occlusion of the internal iliac artery for unrelenting buttock claudication. Catheter Cardiovasc Interv. 2009;74(2):257–259.
42. Brown MD, Gomez-Marin O, Brookfield KF, et al. Differential diagnosis of hip disease versus spine disease. Clin Orthop Relat Res. 2004; (419):280–284.
43. Segal NA, Felson DT, Torner JC, et al.; Multicenter Osteoarthritis Study Group. Greater trochanteric pain syndrome. Arch Phys Med Rehabil. 2007;88(8):988–992.
44. Strauss EJ, Nho SJ, Kelly BT. Greater trochanteric pain syndrome. Sports Med Arthrosc. 2010;18(2):113–119.
45. Williams BS, Cohen SP. Greater trochanteric pain syndrome. Anesth Analg. 2009;108(5):1662–1670.
46. Tibor LM, Sekiya JK. Differential diagnosis of pain around the hip joint. Arthroscopy. 2008;24(12):1407–1421.

Additional Topics: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.

EXTRA IMPORTANT TOPIC: Hip Pain Chiropractic Treatment
Post Disclaimer
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Evaluation of the Patient with Hip Pain" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine; wellness; contributing etiological viscerosomatic disturbances within clinical presentations; associated somato-visceral reflex clinical dynamics; subluxation complexes; sensitive health issues; and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and licensure jurisdiction. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that directly or indirectly relate to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
New Mexico CNP License#: 90560, Verified
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
| Yes | 363LF0000X - Nurse Practitioner - Family | NM |
90560 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
📆 Schedule Appointment: Schedule 24/7 (Click Here)