

As a clinician formally trained in chiropractic and family nursing practice, I have spent years integrating conservative musculoskeletal care with orthobiologic therapeutics grounded in modern evidence-based methods. I’m Dr. Jimenez, DC, FNP-APRN, and in this educational post, I summarize the latest clinical strategies and research trends that guide how I use platelet-rich plasma (PRP), autologous protein concentrates, laser therapy, and shockwave therapy for tendon, joint, and bone-related conditions—focusing on the practical, step-by-step reasoning behind each choice. Over the past decade, the clinical and scientific landscape has shifted dramatically: dedicated organizations like the Interventional Orthobiologics Foundation and the Biologics Association have fostered rigorous, standardized, and patient-centered research methodologies. The result is stronger evidence, clinically meaningful outcomes, and better protocols based on modern bench research and validated patient-reported outcomes (PROs). I aim to offer clinicians and informed patients an approachable yet rigorous window into the clinical decision-making processes that balance efficacy, safety, regulation, and patient experience.
I begin with a granular discussion of how I select and dose protein concentrate (PC) alongside PRP for small- and large-volume joint injections, specifying the rationale for ratios (e.g., 3:1 to 4:1 in volume-restricted joints and 1:1 in larger joints) and when I avoid PC in tendinous applications due to cost-benefit and volume concerns. We will then challenge outdated notions about PRP composition, examining compelling evidence that a small, controlled inclusion of the upper layer of red blood cells—the “red top”—can significantly increase platelet and crucial mononuclear cell concentrations.
Next, I dive into whether and when to employ shockwave therapy following biologic interventions, distinguishing its utility in recalcitrant tendon disorders and bone marrow edema/lesions, while underscoring laser therapy for tenuous, structurally vulnerable tendon presentations. We will transition into the practicalities of application, from appropriate injectate volumes for various joints to the “joint as an organ” concept, which advocates for treating the entire functional joint unit.
From there, I transition to pragmatic practice insights on ethically growing an orthobiologics program without inviting regulatory risk. I outline a framework—the “three-legged stool” of patient trust, regulatory compliance, and practice growth—and detail how the FDA governs products/devices and the FTC governs advertising claims, complemented by oversight from state medical boards. This section offers actionable steps to audit communications and champions evidence-based, balanced messaging over hype. I further articulate a risk-tier framework—the Green Zone, Yellow Zone, and Red Zone—to guide decision-making.
This educational post culminates with detailed procedural walkthroughs, a real-world case study on lateral epicondylitis, and an in-depth look at patient preparation and post-procedure care. The concluding sections—Summary, Conclusion, and Key Insights—recap the central methodologies and reasoning, with explicit dates to anchor timelines and keep the content practically useful. My commitment is to clarity, transparency, and adherence to evolving science—recognizing that best practices grow stronger through ongoing discovery and honest dialogue. This is not medical advice; it is an educational synthesis designed to help clinicians and informed patients understand the mechanisms, methods, and clinical reasoning behind autologous orthobiologic treatments.
Table of Contents
Advancing Orthobiologics: Foundations, Evidence, and Patient-Centered Outcomes
Greetings, and welcome to our educational series on advanced regenerative medicine techniques. I’m Dr. Jimenez, and I’m honored to share my clinical insights and the latest research from our field with you. In my roles as a Doctor of Chiropractic (DC) and a Family Nurse Practitioner (FNP-APRN), I’ve dedicated my practice to integrating evidence-based, cutting-edge therapies to help patients find lasting relief and functional restoration. My approach is rooted in a deep understanding of human physiology and a commitment to leveraging the body’s intrinsic healing capabilities. Today, we’re going to embark on a deep dive into the fascinating world of Platelet-Rich Plasma (PRP) therapy, a cornerstone of modern orthobiologics.
In my practice, I’ve witnessed the transformation of orthobiologics from a niche adjunct into a disciplined, evidence-based arena. Ten years ago, orthobiologics research often relied on heterogeneous methods, limited standardization, and sparse comparative data. Today, with organizations such as the Interventional Orthobiologics Foundation and the Biologics Association spearheading research quality, we’re seeing thoughtful protocols anchored in patient-reported outcomes, validated measures, and preclinical bench research that clarifies mechanisms of action.
- The shift to patient-reported outcomes (PROs) matters because pain, function, and quality of life are the endpoints our patients experience every day. When therapies demonstrate consistent improvements in PROs—alongside objective measures such as imaging or biomechanical testing—our confidence in their clinical effectiveness increases.
- Protocol refinement—covering anticoagulant choice, centrifugation profiles, target volumes, leukocyte modulation, and post-procedural care—has produced more reproducible outcomes. Reproducibility is vital for dose-response clarity and for comparing results across studies and centers.
- Bench research provides mechanistic clarity on growth factor release kinetics, cellular crosstalk in the local microenvironment, and the differential effects of leukocytes across PRP compositions. This knowledge helps us choose the right injectate for tendons, cartilage, or synovium.
The most significant implication of this maturation is the ability to offer patients credible, non-surgical options with realistic expectations of benefit. For many musculoskeletal presentations formerly funneled toward surgery or serial corticosteroid injections, orthobiologics now offer a pathway to correct underlying pathophysiology earlier in the disease continuum, reduce pain, and support native tissue repair.
Why Autologous Therapies Matter: Harnessing the Body’s Repair Systems
Autologous therapies use the patient’s own biologic materials—typically blood or bone marrow components—to mobilize repair mechanisms with lower immunogenic risk and context-appropriate signaling. The core rationale is straightforward: our tissues possess dormant regenerative capacity that can be awakened, focused, and amplified when the right signals and substrates are delivered to the right place.
Key benefits that I observe and target clinically include:
- Accelerated healing through concentrated growth factors that initiate and sustain repair cascades.
- Reduction of pain by modulating inflammatory mediators and improving tissue metabolism.
- Activation of resident adult mesenchymal stromal/stem cells (MSCs) within local niches (peri-tendinous, subchondral, synovial) to promote regeneration.
- Microvascular enhancement (angiogenic signaling) to improve nutrient delivery, waste clearance, and cellular survival under hypoxic stress.
- Stimulation of fibroblast proliferation and collagen synthesis in tendon and ligament applications, restoring structural integrity.
- Coordinated release of key growth factors (e.g., PDGF, TGF-β, VEGF, IGF-1) that manage chemotaxis, cell proliferation, extracellular matrix remodeling, and angiogenesis.
The clinical takeaway: autologous biologics deliver a biologically coherent repair signal. When we understand which signals benefit a particular tissue pathology—and how to deliver them with appropriate composition and dose—we can move beyond generic protocols and into precision biologic care.
The Science of Platelet-Rich Plasma: Debunking Myths and Explaining Mechanisms
Early in my journey, I admittedly considered PRP a kind of “magic dust.” That perception dissolves the moment you engage the basic science. PRP is blood—no more, no less—processed to concentrate platelets and associated bioactive factors. When those platelets degranulate, they release a timed cascade of growth factors and cytokines, stimulating local repair.
Core components in whole blood:
- Plasma and plasma proteins
- Water
- Platelets
- White blood cells (leukocytes)
- Red blood cells (erythrocytes)
Centrifugation separates these by density:
- The top layer: plasma (including platelet-poor plasma, PPP), containing soluble proteins and a fraction of platelets.
- The middle layer: the buffy coat, enriched in platelets and some white blood cells.
- The bottom layer: red blood cells and dense granulocytes (notably neutrophils).
Importantly, platelets straddle layers. Some remain in PPP above the buffy coat; others migrate into the upper RBC stack with neutrophils. This is why recovery is never 100%. It’s also why we design protocols that optimize both yield and composition for the intended application.
The physiologic rationale for PRP:
- Platelet α-granules store PDGF, TGF-β, VEGF, EGF, IGF-1, and other mediators. Upon activation (by collagen exposure, thrombin, calcium, or mechanical stimuli), these mediators deploy rapidly, triggering chemotaxis, proliferation, angiogenesis, and matrix synthesis.
- PRP interfaces with resident MSCs, tenocytes, chondrocytes, synoviocytes, and endothelial cells, orchestrating a networked response tailored by the microenvironment.
- Leukocyte content modulates inflammation. Leukocyte-rich PRP may suit tendon or ligament pathologies requiring a brief inflammatory surge, while leukocyte-poor PRP may suit intra-articular environments where excess inflammation risks chondrotoxicity.
Optimizing PRP Composition: The Evolving Role of Red Blood Cells
A question that frequently arises in both academic circles and clinical training is about the ideal composition of Platelet-Rich Plasma (PRP). Specifically, there has been a significant shift in thinking regarding the inclusion of red blood cells (RBCs). For years, the dogma was to produce the “purest” PRP possible, meaning it was leukocyte-poor and completely devoid of red blood cells. The fear was that RBCs, being pro-inflammatory, would induce a severe post-injection flare, causing unnecessary pain for the patient and potentially hindering the healing process.
However, as our understanding of the cellular dynamics within centrifuged blood has deepened, so has our strategy. The current movement, supported by emerging evidence, is toward the inclusion of a small fraction of the red blood cell layer in our PRP preparation. So, to answer the question directly: In my practice, am I consistently going into the red top of the RBC layer for every patient? The answer is nuanced, but generally, yes, I am. I fine-tune it based on the clinical context, but the default is to capture more of the vital cellular components that lie at that precious interface.
Let’s break down the science behind this decision: when we centrifuge whole blood to create PRP, the components separate by density. At the very bottom, we have the densest components: the red blood cells. Just above them sits a thin, whitish-tan layer known as the buffy coat. This layer is the treasure trove of regenerative medicine. It contains the vast majority of the platelets and leukocytes (white blood cells). Above the buffy coat is the straw-colored platelet-poor plasma (PPP).
The challenge is that these layers are not perfectly distinct. There is a gradient. The highest concentration of platelets and, importantly, the beneficial mononuclear cells—monocytes and lymphocytes—are located in the lower portion of the buffy coat, right at the interface with the red blood cell layer. Monocytes are critical precursors to macrophages, which are the master regulators of the healing process. They orchestrate the cleanup of damaged tissue (M1 phenotype) and then pivot to signal for tissue repair and regeneration (M2 phenotype). Lymphocytes also play a complex, immunomodulatory role in tissue healing.
If we are overly cautious and aspirate only the upper part of the buffy coat to avoid any red color, we are inevitably leaving behind the densest, and arguably most potent, platelets and a significant portion of these crucial mononuclear cells. The research is becoming increasingly clear: a higher concentration of platelets and mononuclear cells correlates directly with greater efficacy and a higher response rate in patients. Therefore, the modern approach involves carefully dipping the aspiration needle just into the top of that RBC layer. The goal isn’t to draw up a large volume of red blood cells, but to ensure we capture the entire buffy coat.
Even with this technique, the final RBC content in the PRP sample is remarkably low, typically less than one percent. So we face a clinical trade-off. Do I prefer a “cleaner” PRP with lower platelet and monocyte concentrations, or do I accept a minuscule number of RBCs to gain a significantly more potent and biologically active injectate? For me, the choice is clear. I will almost always opt for the higher concentration of platelets, monocytes, and lymphocytes.
Now, this doesn’t mean we ignore the potential for an inflammatory flare. For intra-articular injections, particularly in sensitive joints, there is a legitimate concern that even a small number of RBCs can increase hemarthrosis-like irritation and heighten the post-injection inflammatory response. This is where we must be strategic. The inflammatory flare is largely driven by pro-inflammatory cytokines such as Interleukin-1 (IL-1) and destructive enzymes such as Matrix Metalloproteinases (MMPs). The rationale for avoiding RBCs was precisely to minimize this inflammatory onslaught.
Fortunately, we now have sophisticated tools to counteract this. One of the most effective strategies I use is the concurrent injection of an autologous protein concentrate. This is created by passing platelet-poor plasma (PPP), a byproduct of the PRP preparation, through a specialized filter. This process concentrates the large, beneficial proteins naturally present in the plasma. Among these are powerful anti-inflammatory molecules, including Alpha-2-Macroglobulin (A2M) and Interleukin-1 Receptor Antagonist Protein (IRAP).
- Alpha-2-Macroglobulin (A2M) is a broad-spectrum protease inhibitor. Think of it as a molecular “trap.” It binds to and neutralizes the destructive MMPs that degrade cartilage and other tissues.
- Interleukin-1 Receptor Antagonist Protein (IRAP) functions as a competitive inhibitor of IL-1. It binds to the same receptors as the pro-inflammatory IL-1 cytokine but does not activate them. By occupying these receptor sites, it effectively blocks IL-1 from triggering its inflammatory cascade.
By combining our potent, cell-rich PRP with this protein concentrate, we can have the best of both worlds. We achieve powerful regenerative signaling through the high concentration of platelets and mononuclear cells, while simultaneously mitigating potentially excessive inflammatory side effects. We are neutralizing the very molecules (MMPs and IL-1) that underpinned the original fear of including red blood cells. This evidence-based, dual approach allows us to maximize the therapeutic potential of our injectate, leading to significantly better outcomes for our patients.
Evidence-Based Use of PRP and Protein Concentrate in Orthobiologics: Ratios, Indications, and Rationale
In my practice, I continually assess whether adding a protein concentrate (PC) to platelet-rich plasma (PRP) meaningfully improves outcomes for a given tissue target. The central question is not simply, “Does PC help?” but, “Does PC help here now, given this tissue’s mechanics, vascularity, and the patient’s clinical goals?” This decision hinges on biological context, mechanical load expectations, and joint volume constraints.
- Key principle: I reliably use PC in intra-articular joints to augment the bioactive milieu when volume and diffusion can be managed without compromising joint function. In tendons, I do not always use PC. The added volume and cost must be justified by evidence and the clinical scenario.
- Lateral epicondylitis (LE) example: I consistently achieve excellent outcomes with PRP alone. LE’s pathology typically involves microtearing and degenerative changes in the extensor carpi radialis brevis (ECRB) origin, where PRP’s concentrated growth factor profile—particularly PDGF, TGF-β, VEGF, IGF-1, and FGF—targets cellular proliferation, angiogenesis, collagen synthesis, and remodeling. Adding PC raises costs and injectate volume at the tendon-bone interface without always delivering a proportionate benefit. This is why my default is PRP alone for LE, reserving PC for select scenarios.
- Volume-restricted joints: In small joints (e.g., wrist, metacarpophalangeal, thumb CMC), fluid capacity is limited. Excess volume can cause pressure spikes, pain, and suboptimal dispersion. My usual approach employs a 3:1 or 4:1 PRP-to-PC ratio, using a small aliquot of PC to fine-tune the protein environment while respecting volume constraints. The physiologic rationale is to enhance ECM signaling without overwhelming small capsules. For larger joints (e.g., knee, shoulder, hip), I deploy a 1:1 PRP-to-PC ratio when clinically indicated. The broader synovial spaces distribute proteins more evenly, permitting equimolar strategies that reinforce chondral/nociceptive modulation and modulate synovitis without undue pressure.
- Tendon-specific considerations: In tendons, particularly when pathology is tendinosis rather than acute tendinitis, the goal is to shift the matrix from disorganized type III collagen toward aaligned typeI collagen with appropriate cross-linking. PRP alone can catalyze tenocyte proliferation and MMP/TIMP rebalance. PC inclusion may be considered in recalcitrant tendinopathy with poor response to prior PRP, but I weigh the risk of needle trauma, local pressure effects, and cost-equity. In general, a minimally sufficient biologic stimulus, aligned with mechanical loading protocols, produces durable remodeling without excessive injectate.
- Mechanistic notes: PC can provide additional albumin, globulins, anti-protease elements, and cytokine-modulating proteins that potentially dampen catabolic enzymes and reduce inflammatory noise. However, the net biological impact is context-dependent. Tendon microenvironments with low vascularity and dense ECM resist dispersion; optimizing injection technique (peppering vs. fenestration), ultrasound guidance, and post-procedure loading often matters more than adding PC volume.
Bottom line: Intra-articular applications frequently benefit from PC adjuncts; tendinous applications often perform well with PRP alone—particularly in LE—unless clinical features and prior outcomes argue otherwise.
Precision in Practice: A Guide to Joint-Specific Injection Volumes
When administering orthobiologic injectables like PRP, one of the most critical factors for success and patient comfort is the injection volume. It’s a common misconception to think that “more is better.” In reality, each Joint in the human body is a distinct biomechanical environment with a specific synovial capacity. Exceeding this capacity, or over-distending the joint capsule, can be intensely painful in itself, creating iatrogenic pain that can be mistaken for a severe inflammatory flare or procedural failure. It can also potentially damage the delicate synovial lining. Therefore, a “one-size-fits-all” approach is not just suboptimal; it’s poor medical practice. My injection volumes are carefully tailored to the specific joint being treated, based on anatomical constraints and clinical experience.
Let’s walk through a general guideline of the volumes I use in my practice. Please remember these are starting points and can be adjusted based on patient size, the specific pathology, and intra-procedural feedback.
Large Volume Joints: Knees and Shoulders
The knee and the glenohumeral Joint (shoulder) are considered large-volume synovial joints. They have a relatively lax and capacious joint capsule that can comfortably accommodate a larger volume of fluid.
- Knees & Shoulders: For these joints, I am very comfortable injecting up to ten cubic centimeters (10 ccs) of total injectate. This volume is generally well tolerated and allows for thorough coating of the articular surfaces and distribution of PRP throughout the synovial space. In the knee, this volume ensures that the biologic can reach all three compartments (medial, lateral, and patellofemoral). In the shoulder, it allows the injectate to access the humeral head, the glenoid, and the long head of the biceps tendon where it passes through the Joint.
Medium Volume Joints: Hips and Ankles
The hip and ankle joints are more constrained and have a significantly smaller intra-articular volume compared to the knee or shoulder. Overfilling these joints can quickly lead to a painful pressure spike.
- Hips: The hip joint is a deep, congruent ball-and-socket joint with a very strong and relatively tight fibrous capsule. For an intra-articular hip injection, I limit the total volume to four to five cubic centimeters (4-5 cc). This is typically sufficient to treat the articular surfaces without causing painful capsular distension.
- Ankles: The tibiotalar Joint, or ankle joint proper, is also a smaller-volume space. For ankle injections, I am usually in the two to three cubic centimeter (2-3 cc) range. This provides adequate treatment for conditions like ankle osteoarthritis or osteochondral defects while respecting the Joint’s limited capacity.
Small Volume Joints: Elbows, Wrists, and Digits
As we move to the smaller joints of the upper extremity, the permissible volumes decrease even further. These joints are intricate and have very little tolerance for excess fluid.
- Elbows: The elbow (humeroulnar and humeroradial articulations) is a hinge joint with a snug capsule. Similar to the ankle, my typical volume for an intra-articular elbow injection is two to three cubic centimeters (2-3 ccs).
- Wrists: The wrist is a complex region with multiple small articulations (e.g., the radiocarpal Joint). Here, the volume is even more restricted. I generally use one to two cubic centimeters (1-2 ccs) for wrist injections.
- Fingers & Toes (Metacarpophalangeal, Interphalangeal Joints): These small digital joints can rarely hold more than one cubic centimeter (1 cc). Often, the volume is even smaller.
- Acromioclavicular (AC) Joint: The AC joint in the shoulder is another very small synovial joint. An injection here might only accommodate 75 cubic centimeters (0.75 cc) or even less.
Adhering to these volume guidelines is crucial to procedural safety and efficacy. The goal is to deliver a therapeutic dose of the biologic directly to the target tissue without causing harm or undue discomfort from mechanical pressure.
The “Joint as an Organ” Concept: A Comprehensive Treatment Approach
A pivotal concept in modern regenerative orthopedics is treating the “joint as an organ.” This paradigm shift moves us away from the reductionist view of treating a single, isolated structure (e.g., only the cartilage inside the Joint) and towards a more holistic, functional approach. A joint is not merely two bones meeting; it is a complex, integrated system composed of cartilage, synovium, subchondral bone, the joint capsule, stabilizing ligaments, and the tendons and muscles that cross it. Pain and dysfunction often arise from a failure in multiple components of this system, not just one.
So, when a patient asks if the injection volumes I mentioned are just for the intra-articular space and if I use the rest of the PRP elsewhere, the answer is a resounding yes, absolutely. My approach is nearly always comprehensive. The volume I inject intra-articularly is specifically for that space. The remaining PRP or protein concentrate is then meticulously used to treat the extra-articular ligamentous and tendinous structures that are critical to the Joint’s stability and function.
This is what some refer to as the functional joint unit approach. For example, when treating a knee, I don’t just inject into the joint space. I will also assess and treat the medial collateral ligament (MCL), the lateral collateral ligament (LCL), the pes anserine tendons, and the patellar tendon if they are tender, lax, or show pathology on diagnostic ultrasound. In the shoulder, this means addressing the rotator cuff tendons, the coracoacromial ligament, and the capsular ligaments.
This comprehensive strategy is especially vital for patients with any form of joint instability. This is particularly true for my patients with Ehlers-Danlos Syndrome (EDS) or other hypermobility spectrum disorders. In these individuals, the primary pathology is often ligamentous laxity. The ligaments, which act as the Joint’s static stabilizers, are too stretchy and fail to provide adequate support. This leads to micro-instability, chronic pain, and eventually, secondary damage to the cartilage and other structures. In these cases, simply injecting PRP into the joint space without addressing the failing ligaments is treating a symptom, not the root cause. My protocol involves a thorough evaluation of the joint capsule and all relevant ligaments, followed by targeted injections (prolotherapy-style) into these structures to stimulate a fibroblastic response, encouraging them to tighten and strengthen over time.
By treating the entire functional unit—the Joint and its supporting soft tissues—we create a more stable and biomechanically sound environment. This not only addresses multiple pain generators simultaneously but also protects the intra-articular environment from the ongoing damage caused by instability. It is a more thorough, more logical, and ultimately, more effective way to achieve long-term positive outcomes for our patients.
Modern PRP Processing: Protocols, Precision, and Reasoning
In my clinic, I employ a single-spin, benchtop processing workflow designed to balance simplicity and control. The goals are consistent platelet recovery, adjustable leukocyte content, and reproducible volumes tailored to the target tissue.
Workflow fundamentals:
- Anticoagulation: I use ACD-A to prevent premature platelet activation and maintain flow characteristics during draw and processing.
- Blood draw: Typically via a 19-gauge butterfly needle, collecting up to 60 mL total (including 6 mL ACD-A).
- Gentle inversion: Approximately 15 inversions to ensure anticoagulant mixing, preventing microclots that would disrupt separation.
- Counterbalancing: Device mass is matched to within 1 g using water calibration to avoid rotor imbalance, thereby preserving separation integrity and device safety.
- Centrifugation: A single 10-minute spin at approximately 3500 RPM (a PRP 60 profile) reliably separates RBCs, buffy coat, and plasma. This speed/time pairing achieves a robust interface while limiting shear forces that could damage platelets.
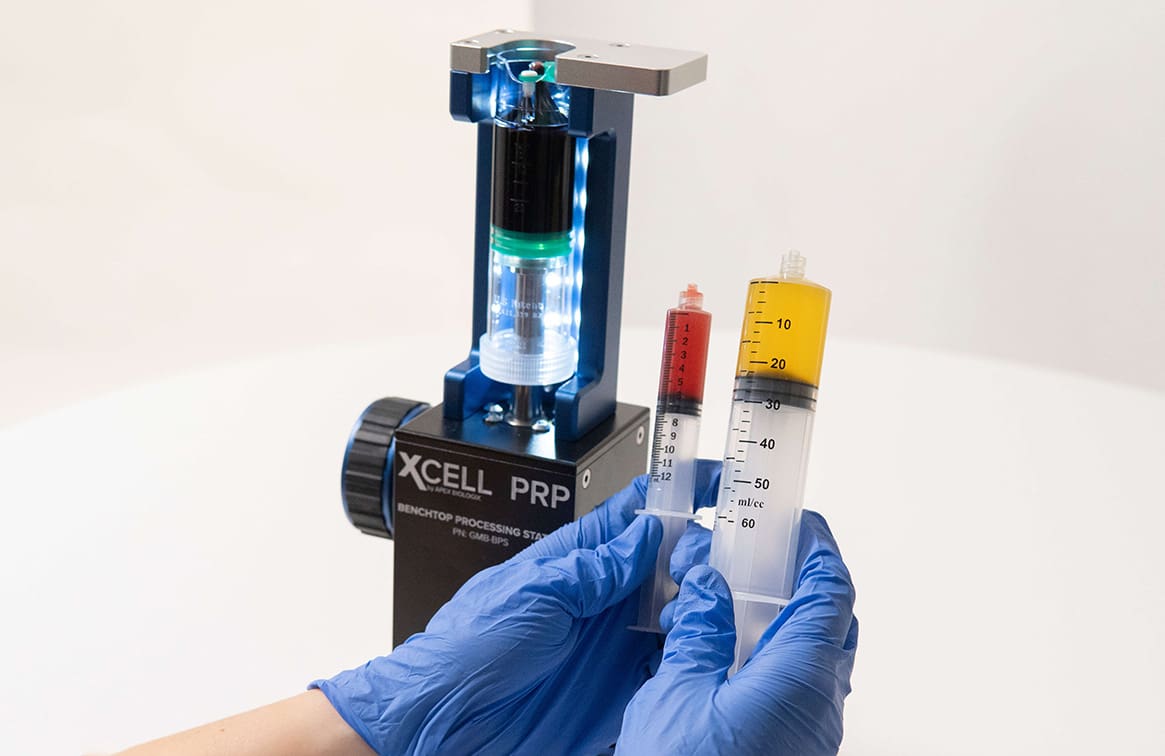
- Buffy coat capture: The benchtop station allows controlled advancement of plasma, stopping at the 6–7 mL mark where the buffy coat begins, then switching syringes to capture it with precision. This yields a target volume of approximately 6–7 cc PRP for many applications.
Why each step matters:
- Anticoagulant choice and mixing ensure platelets remain intact and inactive until delivered to the tissue, preserving growth factor payload.
- Single-spin protocols reduce complexity and cumulative shear stress, supporting better platelet function on injection.
- Visual interface management (lighted benchtop station) improves accuracy in identifying layer transitions, reducing RBC contamination.
- Volume targeting aligns dose (total platelet count) with the target lesion’s biology and size, avoiding overdilution and ensuring sufficient bioactivity.
Leukocyte modulation:
- The system enables customization of leukocyte content. In some cases, I reduce granulocytes to temper catabolic protease and ROS activity, particularly in intra-articular environments. In other cases—chronic tendinopathy with a disorganized matrix—a modest leukocyte presence can facilitate an initial inflammatory phase that kickstarts remodeling.
Quantifying PRP: Dose, Recovery, and Composition
 Quantification is central to modern orthobiologics. I measure baseline whole-blood counts and PRP outputs using a hemocytometer or an automated analyzer. This informs the total platelet dose, recovery percentage, and leukocyte profile.
Quantification is central to modern orthobiologics. I measure baseline whole-blood counts and PRP outputs using a hemocytometer or an automated analyzer. This informs the total platelet dose, recovery percentage, and leukocyte profile.
Example data from my clinic:
- Baseline platelet count in the 200s x10^9/L
- PRP output concentration around 2128 x10^9/L (per L equivalent), with 7 cc final volume
- Total platelet dose: approximately 14.89 billion platelets in the 7 cc PRP syringe
- Recovery: ~94% in the sample highlighted, an excellent yield
- Granulocyte reduction: achieved when clinically indicated, based on tissue and application
Why dose matters:
- Platelet dose correlates with growth factor availability. In under-dosed PRP, therapeutic thresholds may not be reached; in over-dosed compositions, excessive viscosity or activation may impede delivery or cause undue irritation.
- Dose and composition drive outcomes. The literature increasingly supports dose standardization for specific indications (e.g., lateral epicondylitis, knee osteoarthritis), enhancing comparability across centers.
Color and RBC content:
- Slight pink or red hue often indicates minimal RBC presence; it takes very little hemoglobin to tint the sample visually. This does not necessarily reflect significant RBC contamination if counts remain low.
- Control of the interface during buffy coat capture is fundamental to minimize RBCs while retaining platelets.
Anesthesia Protocols: Balancing Patient Comfort and Biological Efficacy
The topic of local anesthesia in regenerative procedures requires careful consideration. The primary goal of our PRP injection is to initiate a robust, natural inflammatory and healing cascade. Certain local anesthetics, particularly those in the “-caine” family like Lidocaine and Bupivacaine, have been shown in laboratory studies to be chondrotoxic (toxic to cartilage cells) and potentially myotoxic (toxic to muscle cells). There is also evidence to suggest they can impair platelet function and blunt the very inflammatory response we are trying to create. Therefore, the decision of whether, when, and what type of anesthetic to use is not trivial. My protocol is designed to maximize patient comfort while minimizing potential interference with the treatment’s biological efficacy.
My approach to local anesthesia is bifurcated, depending on the location of the injection:
Intra-Articular Injections: No Local Anesthetic
For injections that are purely intra-articular (inside the joint capsule), I do not use any local anesthetic mixed in with the PRP. The primary reason is to avoid any potential chondrotoxic effects on the cartilage we are trying to heal and to prevent any blunting of the platelet-driven healing cascade. Patients generally tolerate intra-articular injections well, as the joint space itself has relatively few nerve endings compared to the surrounding soft tissues. The discomfort is brief and manageable.
Extra-Articular Injections: Strategic Use of Low-Dose Ropivacaine
The situation is entirely different for extra-articular injections, which involve treating tendons, ligaments, and other soft tissues. These structures are richly innervated, and injections into them can be quite painful. My goal is to ensure the patient has a tolerable experience and walks out of the office not cursing my name. I’ve learned from experience that performing extensive extra-articular work without any anesthetic can be an excruciating experience for the patient, which can create anxiety about future treatments and follow-up.
For these soft tissue applications, I use a very low-dose, low-volume ropivacaine. Specifically, I use a 0.125% concentration by volume. I choose ropivacaine for several reasons. First, studies suggest it is less chondrotoxic and myotoxic compared to bupivacaine and lidocaine. Second, it has a longer duration of action, providing the patient with sustained relief for several hours after they leave the clinic. The concentration is key. By using a very dilute 0.125% solution, I am aiming for a sensory block (pain relief) without a significant motor block and, importantly, minimizing the total anesthetic dose to limit any potential negative impact on the regenerative process. This small amount of relief makes the procedure vastly more tolerable, improving the overall patient experience without, in my clinical experience, compromising the excellent outcomes we see.
So, to summarize my protocol:
- Intra-articular: No local anesthetic mixed with the injectate.
- Extra-articular (tendons, ligaments): A very low concentration (0.125%) of ropivacaine is used in the soft tissue to manage procedural pain and ensure patient comfort.
This balanced approach respects the biology of the treatment while also respecting the patient’s need for a comfortable and positive clinical experience.
Managing the Healing Process: The Truth About the Inflammatory Flare
One of the most important concepts to communicate to patients undergoing PRP therapy is the nature of the post-injection experience. A common question I get is, “How can we mitigate the inflammatory flare response?” This question often comes from a place of fear, as both patients and practitioners are conditioned to view inflammation as something negative that must be suppressed. However, in the context of regenerative medicine, this view is fundamentally misguided.
The entire goal of injecting PRP is to restart the body’s natural healing cascade. Chronic injuries, like tendinopathy or osteoarthritis, are stuck. The normal healing process has stalled, often in a state of chronic, low-grade, degenerative inflammation. PRP acts as a powerful biological signal that essentially tricks the body into thinking a new, acute injury has occurred. This initiates a robust acute inflammatory response, which is the first and absolutely essential phase of healing.
Think about what happens when you sprain your ankle. It becomes swollen, red, warm, and tender. This is the acute inflammatory response in action. It’s the body rushing blood flow, growth factors, platelets, and immune cells to the area to clean up damage and lay the groundwork for repair. We want this to happen after a PRP injection. Suppressing this acute, productive inflammation with anti-inflammatory drugs would be like calling the fire department to an injury and then telling them to go home before they’ve put out the fire and cleared the debris.
So, when patients ask how we can “mitigate” the flare, my first step is education. I reframe the flare not as a side effect to be avoided, but as an indicator that the treatment is working. It’s a sign that we have successfully initiated the healing cascade. The sequence we are aiming for is: Acute Inflammation → Proliferation → Remodeling → Full Resolution and Tissue Healing. The PRP kickstarts this process.
That being said, we don’t want the patient to be in agony. The goal is not to eliminate the flare but to help the patient manage symptoms and potentially shorten the duration of the most uncomfortable phase. I use a multi-pronged approach for symptom relief and to support the healing process:
- Protein Concentrate: As discussed earlier, one of my primary tools is the concurrent use of an autologous protein concentrate rich in A2M and IRAP. This is a biological, not a pharmaceutical, way to manage the flare. It doesn’t stop the beneficial inflammatory signaling; rather, it neutralizes the excessively destructive components like proteases (MMPs) and the potent inflammatory cytokine IL-1. This helps to balance the inflammatory environment, reducing pain and protecting tissues without shutting down the healing process.
- Bioactive Compression Sleeves: Immediately after the procedure, I provide my patients with a bioactive sleeve. The brand I currently use is the Reparel® This is similar to other products made from “cell-responsive” fabrics. These garments are woven with minerals that capture the body’s natural heat and convert it into infrared energy, which is then reflected back into the tissues. This is thought to increase local circulation and oxygenation. Clinically, I find these sleeves are excellent for reducing pain, swelling, and inflammation. They help to accelerate the patient’s journey through the inflammatory curve, not by stopping it, but by making the process more efficient.
- MLS Laser Therapy: I am a strong proponent of MLS (Multiwave Locked System) Laser Therapy as an adjunctive modality. This is a Class IV laser that uses specific, synchronized wavelengths of light to penetrate tissue and stimulate cellular activity. It has a dual effect: it’s both anti-inflammatory and analgesic (pain-relieving). Like the bioactive sleeve, the goal of laser therapy is not to quash the inflammatory cascade but to accelerate it. It helps to speed up the transition from the pro-inflammatory M1 macrophage phase to the pro-resolving M2 macrophage phase. I have my patients come in for at least three laser sessions during the first week post-injection. This significantly helps with pain and swelling and compresses the time the patient spends in that initial, uncomfortable phase..
- Splinting and Medication (As Needed): For certain procedures, especially in the extremities, I may place the patient in a splint for overnight use for the first few days to rest the area and minimize pain from movement during sleep. In cases of very extensive procedures or for patients with a very low pain threshold, I will provide a very short course of narcotic pain medication—typically just enough for 24 to 48 hours—to help them get through the peak of the discomfort.
By combining patient education with these supportive therapies, we can successfully manage the post-procedural experience, ensuring the patient is comfortable while allowing the essential biological process of healing to unfold unimpeded.
Setting the Stage for Success: The Pre-Procedure Protocol
The success of a regenerative medicine procedure begins long before the needle ever touches the skin. A thorough and meticulous pre-procedure protocol is essential to optimize the patient’s physiology for healing, set clear expectations, and ensure safety. My pre-procedure consultation is a non-negotiable, comprehensive discussion lasting at least 30 minutes. During this time, we leave no stone unturned. Here is a breakdown of the key components of my pre-procedure discussion and preparation instructions.
Medication Management
- Anti-Inflammatory Medications (NSAIDs): This is a critical point of discussion. Medications like ibuprofen, naproxen, and their prescription counterparts work by inhibiting the COX enzymes, which are instrumental in producing the prostaglandins that drive the inflammatory response. Since our goal with PRP is to induce this very response, the continued use of NSAIDs is counterproductive and can blunt or even negate the effects of the treatment. I require patients to discontinue all anti-inflammatory medications for at least one week before the procedure, and preferably longer. If a patient is on a daily NSAID for chronic pain management and cannot simply stop, I will often transition them to meloxicam. While still an NSAID, evidence suggests that meloxicam may be less disruptive to the specific pathways involved in regenerative signaling; it appears to “play nicest in the sandbox” with orthobiologic therapies compared to other NSAIDs. However, the ideal scenario is for the patient to be off all NSAIDs.
- Steroid Injections: If a patient has recently had a corticosteroid injection in the area we plan to treat, this is a hard stop. Corticosteroids are catabolic (they break down tissue) and are profoundly anti-inflammatory. They can suppress the local cellular activity needed for healing for an extended period. I require a washout period of at least six to eight weeks between a steroid injection and a PRP procedure.
- Blood Thinners (Anticoagulants and Antiplatelets): This is a complex issue that requires careful, individualized management. A few weeks ago, we had an in-depth discussion on this topic. The decision to stop a blood thinner depends on several factors: the specific medication and its mechanism of action, the reason it was prescribed (the patient’s underlying thrombotic risk), and the nature of the procedure. You must collaborate with the prescribing physician to assess the risks of stopping the medication versus performing the procedure while on it. For example, stopping a blood thinner for a patient with a mechanical heart valve or recent pulmonary embolism carries a very high risk. If the risk of stopping is too high, the procedure can often still be performed, but it’s not a hard “no.” There are strategies to manage it, but it requires careful risk stratification and interdisciplinary communication. If the medication can be safely discontinued, we follow standard protocols for the specific drug.
Lifestyle and Dietary Optimization
- Hydration: This is simple but absolutely crucial. A well-hydrated patient has plump, easily accessible veins and healthier plasma. Dehydration leads to viscous blood, making the blood draw difficult and potentially compromising the quality of the PRP. I instruct my patients to begin actively hydrating—drinking plenty of water—two days before the procedure.
- Caffeine: I advise patients to stay away from significant amounts of caffeine on the day of the procedure. Caffeine is a vasoconstrictor, meaning it can clamp down blood vessels, making the blood draw more difficult. I once had a young, healthy patient who had consumed three Monster energy drinks before his appointment. His veins were so constricted that I could not get a successful blood draw. He had to be rescheduled for the next day.
- Diet and Fasting: The question of whether to eat or fast before a procedure is common. From a safety perspective, if a patient is prone to vasovagal episodes (fainting), it is essential that they eat a meal to maintain stable blood sugar levels. However, from a biological optimization standpoint, there is some emerging evidence to suggest that intermittent fasting in the 12-16 hours leading up to the procedure may be beneficial. Fasting can upregulate autophagy (the body’s cellular cleanup process) and may help to mobilize mesenchymal stem cells from the bone marrow into the peripheral circulation, potentially enriching the final PRP product. This is an area of ongoing research, but it’s a promising strategy for patients who can tolerate it.
- Smoking and Alcohol: These are absolute contraindications around the time of the procedure. Both smoking and alcohol are directly cytotoxic (toxic to cells). Nicotine is a potent vasoconstrictor that starves tissues of oxygen and healing nutrients. Alcohol can impair liver function, which is critical for producing the proteins needed for healing, and can also have direct negative effects on cellular function. I require patients to abstain from smoking and drinking alcohol during the treatment and recovery period.
Administrative and Financial Clarity
It is imperative to be transparent about the financial aspects of the procedure. Most regenerative medicine therapies are not covered by insurance.
- Informed Financial Consent: We clearly outline the total price of the procedure, what that cost includes (consultation, the procedure itself, follow-up visits, adjunctive therapies such as laser), and our payment policies.
- Advanced Beneficiary Notice (ABN): For any patient who is a Medicare beneficiary, it is a legal requirement to have them sign an Advanced Beneficiary Notice of Noncoverage (ABN). This is a formal document stating that the patient understands that Medicare will not cover the procedure and that they personally accept full financial responsibility. This protects the practice and ensures the patient is fully informed that they cannot and will not seek reimbursement from Medicare.
A thorough pre-procedure protocol is the foundation for a successful outcome. It optimizes the patient’s biological canvas, manages risks, and establishes a strong, transparent therapeutic alliance.
Case Study: Ultrasound-Guided PRP for Lateral Epicondylitis
To truly understand the application of these principles, let’s walk through a real-world case. This patient is a lovely dental assistant who presented with chronic right lateral epicondylitis, or “tennis elbow.” Her occupation involves repetitive wrist and forearm movements, a classic risk factor for this condition. Before seeing me, she had already tried a host of conservative treatments, including NSAIDs, counterforce braces, and acupuncture, with no lasting relief. Notably, she had undergone a single PRP injection previously, but it was performed “blind” (without ultrasound guidance), and she was unsure of the cell dose or concentration she received. Her continued pain suggested the previous treatment was either misplaced, under-dosed, or both.
Diagnostic Ultrasound
The first step is always a thorough diagnostic ultrasound examination. This allows me to visualize the anatomy in real-time and confirm the diagnosis and the extent of the pathology. I have the patient lay supine with her arm resting comfortably. After palpating the area of maximal tenderness over the lateral epicondyle, I place the ultrasound transducer in a long-axis orientation relative to the common extensor tendon.
What we immediately see on the screen is a classic picture of severe tendinopathy. The normal, bright, fibrillar pattern of a healthy tendon is replaced by dark, hypoechoic areas, particularly at the insertion point on the lateral epicondyle. This hypoechogenicity represents a disorganized, degenerative, and sometimes fluid-filled or torn tissue. In her case, the pathology is significant, indicating a substantial partial-thickness tear involving at least a third, and in some areas, up to two-thirds of the tendon’s thickness. This objective finding confirms that she is an excellent candidate for PRP and explains why her previous therapies failed.
The Injection Procedure: Technique and Nuances
After confirming the pathology, I plan my injection. I use an in-plane, long-axis approach, meaning the needle will be inserted parallel to the ultrasound transducer, and I will be able to see the entire length of the needle, from shaft to tip, throughout the procedure. My entry point will be from the right side of the screen (distal to the elbow), advancing the needle toward the epicondyle.
- Bending the Needle: Here is a little trick I love to use for superficial targets like this. I take the sterile needle and give it a single, gentle bend of about 15-20 degrees. You can only do this once; bending it back and forth will weaken the metal and increase the risk of breakage. This “hockey stick” bend allows the needle to lie more parallel to the skin surface, making it easier to visualize with the ultrasound transducer while still allowing the tip to be angled down into the target tissue. It provides much better control and visualization.
- Initial Pass and “Peppering”: I advance the needle through the subcutaneous tissue until the tip is positioned directly over the most significant hypoechoic area within the tendon. I then gently advance the tip down into the tear. Now I begin injecting the PRP. My technique is called “peppering” or fenestration. I don’t simply deposit a single large bolus of fluid. Instead, I make multiple small passes with the needle tip throughout the entire area of diseased tissue, depositing small aliquots of PRP with each pass. This serves two purposes:
- It mechanically breaks up the degenerative, scar-like tissue, stimulating a small amount of bleeding and initiating a healing response even before the PRP gets to work.
- It ensures a much more even and thorough distribution of the platelets and growth factors throughout the entire volume of the damaged tendon.
You can see on the video as I inject, the dark, torn area begins to fill with the PRP, lifting the tendon fibers apart. This confirms I am in the correct location. It is a large tear, and as I am performing the injection, I am having a conversation with the patient, managing expectations in real-time. I’ll say something like, “Wow, this is a pretty significant tear I’m seeing here. It’s important you are diligent with your post-procedure care. Some injuries of this size may require more than one treatment.”
- Switching to a Short-Axis View: After thoroughly peppering the tendon in the long-axis view, I rotate the ultrasound transducer 90 degrees into a short-axis, out-of-plane view. In this view, the tendon looks like an oval, and the needle appears as a bright, hyperechoic dot. This view is invaluable because it allows me to confirm the depth of my needle tip. I can see if I am in the superficial, mid, or deep portion of the tendon. This ensures I have treated the full thickness of the pathology from top to bottom, not just front to back. As I inject in this view, I can see the entire tendon lifting up, which gives me great confidence that the PRP is being delivered exactly where it needs to be.
- Dose is Key: I continue peppering the tissue until I have used the entire syringe, which in this case contains about three cubic centimeters (3 ccs) of super-concentrated PRP. This PRP was prepared by taking only the buffy coat as it is aspirated from the centrifuged blood column. We know from the literature that for soft tissue applications like tendinopathy, dose matters. A landmark paper by Luca Podesta and others has shown that a dose of at least 3.5 billion platelets is a critical threshold. Doses above this level are associated with positive outcomes, while doses below it have limited or unpredictable results. By using a highly concentrated product and delivering a sufficient volume, I am ensuring we meet this therapeutic threshold. I want to give her the absolute best chance of a “one and done” success. It’s also worth noting Podesta’s work, which showed that in patients who initially failed PRP for lateral epicondylitis, a second, properly dosed and placed injection was often successful. This reinforces the idea that initial failures are often a problem of dose or delivery, not a failure of the concept itself.
By combining precise ultrasound guidance, advanced injection techniques like peppering and multi-planar views, and an evidence-based, therapeutic dose of platelets, we can transform a condition that has been refractory to multiple other treatments and offer the patient a genuine opportunity for complete and lasting healing.
Post-Procedure Care and Long-Term Rehabilitation
The 48-72 hours following the procedure are just the beginning of the healing journey. A structured and comprehensive post-procedure protocol is essential for managing symptoms, supporting the biological process, and guiding the tissue back to full function. My post-procedure discussion is as detailed as my pre-procedure one, ensuring the patient is a well-informed and active participant in their own recovery.
As we’ve discussed, I educate the patient to expect significant tenderness and soreness for the first two to three days. This is the acute inflammatory phase, and it is a good sign. My strategy for managing this involves the Reparel® bioactive sleeve, MLS Laser therapy (with a goal of at least 12 sessions between injection and their formal follow-up), topical analgesics, and a short-term splint for nighttime use to rest the tendon.
A crucial aspect of my post-procedure instructions is the strict avoidance of certain substances:
- Anti-inflammatories (NSAIDs): I ask patients to continue to avoid all NSAIDs for several weeks after the injection. We’ve worked hard to create a productive inflammatory response, and we do not want to blunt it with medication.
- Smoking and Alcohol: As mentioned, these are cytotoxic and severely impair healing. I require patients to continue to abstain from smoking and alcohol throughout the recovery period.
The patient is not formally re-evaluated by me until eight weeks post-injection. This time frame is chosen deliberately. The biological healing cascade takes time. The initial inflammatory phase transitions into the proliferative phase (typically weeks 1-6), where the body begins to lay down new, disorganized collagen (Type III). This is followed by the remodeling phase (from week 6 up to a year or more), where this immature collagen is slowly replaced and reorganized into strong, mature, and aligned Type I collagen. Seeing a patient too early can be misleading, as significant healing is still underway.
However, “no follow-up for eight weeks” does not mean no contact. The patient has at least twelve touches with my team during their laser therapy sessions. My staff is trained to monitor their progress, answer questions, and escalate any concerns to me. We also use data collection tools to track their pain scores and functional improvement throughout this period.
Rehabilitation: The Tendon Training Program
Perhaps the most critical component of long-term success, especially for tendinopathy, is a structured rehabilitation program. I typically have my patients begin formal physical therapy about two weeks after the injection. We start with gentle range of motion exercises right away to prevent stiffness. However, the core of the rehab is the tendon rehab protocol.
I explain this to my patients as a “tendon training program.” Tendons are designed to withstand and transmit heavy loads. A healed tendon must be retrained to do its job effectively. The rehab protocol focuses on progressive eccentric and heavy slow resistance training.
- Eccentric loading refers to contracting the muscle while it is lengthening (e.g., slowly lowering a weight). TTypetype of loading has been shown to be particularly effective at stimulating collagen synthesis and remodeling in tendons.
- Heavy slow resistance training involves using challenging weights and moving through the range of motion very slowly.
This mechanical stress is not harmful; it is a vital signal. As we move through the proliferative and remodeling phases of healing, applying this controlled, progressive load guides the new collagen fibers to lay down in a highly organized, parallel alignment. This is what creates a tendon with high tensile strength, capable of resisting the forces of daily activity and sport. Without this mechanical guidance, the new tissue can heal as a disorganized scar, which is weak and prone to re-injury. The physical therapy program is essential for translating the biological healing initiated by the PRP into a functional, durable, and resilient tissue.
Follow-Up and Redosing Strategy: Defining Success
A critical part of managing patient expectations and clinical decision-making is having a clear follow-up and redosing strategy. When a patient undergoes a PRP procedure, a common question is, “When will I need to have this done again?” My honest answer is, “I hope never.” The goal and plan for a high-concentration, precisely delivered PRP injection is “one and done.” We aim to provide a sufficiently powerful stimulus to restart the healing cascade, leading to a durable, long-term resolution of the problem.
However, biology is complex, and not every patient responds in the same way. This is why having a clear benchmark for success is crucial. As I mentioned, my first formal clinical reassessment is at the eight-week mark post-injection. At this visit, I perform a thorough physical exam and, most importantly, I quantify the patient’s improvement. My key benchmark is a fifty percent (50%) improvement in pain and/or function by eight weeks.
- If the patient has achieved 50% or greater improvement: This is a fantastic sign. It tells me that they are a good responder and that the healing trajectory is well on its way. The remodeling phase of healing will continue for many more months, so we expect their improvement to continue to build upon this foundation. In this case, we continue with the rehabilitation plan and no further injection is considered at this time.
- If the patient has achieved less than 50% improvement: This is the point where I begin to consider redosing. A suboptimal response does not necessarily mean the therapy has failed. In fact, there is good literature, particularly in the field of knee osteoarthritis, that provides a strong rationale for a second injection. Studies have shown that among patients who are classified as “non-responders” to an initial PRP injection, approximately 75% of them can be converted to responders with a second dose.
This strongly suggests that many initial “failures” are not a failure of the patient to respond to the therapy, but rather a dosing problem. The initial dose may have been insufficient to overcome the catabolic environment of their chronic condition. When a patient asks what “redosing” means—if I use a double dose—the answer is no, I don’t change the concentration. I simply do it again. I administer another full, therapeutic dose of high-concentration PRP.
It is important to note that I do not tell my patients about this redosing option upfront. I don’t want to plant the seed in their mind that they will likely need two treatments. I want them to be fully committed to the goal of a single, successful procedure. However, I hold this option back as a clinical tool, at my discretion, for the subset of patients who show a partial but insufficient response at the eight-week mark. This strategy allows us to salvage a positive outcome for a significant number of patients who might otherwise be considered treatment failures.
Lateral Epicondylitis: PRP Alone, Loading Timelines, and Return-to-Play Rationale
 I have personally undergone PRP for tendon pathology and empathize deeply with the recovery trajectory, especially for high-demand individuals. When patients—often tennis players—ask when they can resume play, my answer is grounded in tissue biology and staged loading.
I have personally undergone PRP for tendon pathology and empathize deeply with the recovery trajectory, especially for high-demand individuals. When patients—often tennis players—ask when they can resume play, my answer is grounded in tissue biology and staged loading.
- Pain and tissue response: PRP induces an acute inflammatory phase, followed by proliferation and remodeling. Expect soreness early as inflammatory mediators recruit cellular machinery. The subsequent phase requires controlled mechanical stimulus to align collagen fibers and mature the ECM.
- Typical timeline: Many high-demand individuals can resume heavier activities around 7–10 days post-PRP if baseline pathology is moderate and their mechanics are sound. However, severity and chronicity dictate caution. For more advanced LE cases, I delay tennis for several weeks to allow adequate substrate deposition (collagen scaffolding) and reduce the risk of setback. Biological healing is not strictly linear; early overload can disorganize nascent fibers.
- Loading program: I structure loading around isometrics first (pain-modulated intensity at mid-range positions), progressing to eccentrics (to stimulate tendon remodeling with controlled strain) and then to concentric and plyometric components as tolerated. Evidence supports isometric work for analgesia via central and peripheral pathways—reducing pain while priming the tendon. Eccentrics drive mechanotransduction—upregulating tenocyte activity, collagen synthesis, and cross-link integrity.
- Technique choices: I favor ultrasound-guided infiltration to target the ECRB enthesis precisely, minimizing extratendinous dispersion and iatrogenic trauma. Peppering techniques distribute PRP microdroplets across degenerated zones, improving local bioavailability. I coach strict avoidance of provocative drills until pain at rest and pain during isometrics are within acceptable thresholds (usually ≤3/10).
- Why PRP alone: For LE, randomized controlled trials and systematic reviews have demonstrated benefit from PRP over corticosteroid in medium-term outcomes, improving pain and function and reducing recurrence. PC’s incremental mechanistic advantage remains less clear in this tendon context; the marginal utility often does not justify additional injectate. Practical experience aligns: PRP’s growth-factor milieu is typically sufficient to guide a degenerative tendon toward recovery when paired with disciplined loading and ergonomics.
- Return-to-play specifics: We stage tennis reintroduction—beginning with short sessions, low-intensity strokes, and modified grips to minimize lateral elbow strain. We integrate forearm conditioning, proximal kinetic chain optimization (scapular stabilizers, rotator cuff, trunk rotation), and racket modifications (string tension, grip size) to reduce lateral epicondylar load. Grip technique (avoiding overgrip, maintaining neutral wrist) is crucial.
Patient education: Expect tenderness early, respect tissue biology, and embrace graded loading. The outcome hinges as much on what happens post-injection as the injectate itself.
Shockwave Therapy Post-PRP: Indications, Timing, and Tissue-State Strategy
Shockwave therapy—both focused (fESWT) and radial (rESWT)—delivers controlled mechanical energy that can modulate pain and stimulate tissue regeneration. The decision to use shockwave post-PRP depends on the tissue’s mechanical resilience, structural integrity, and sensitization status.
- When I hold off: In tenuous tendon states (significant structural compromise, heightened irritability) or in patients with central sensitization, I delay shockwave. The mechanical stimulus can be perceived as nociceptive overload, potentially amplifying pain pathways and undermining early healing.
- Preferred first-line in tenuous tendon: I begin with laser therapy (e.g., photobiomodulation) to downregulate inflammatory mediators, support mitochondrial function (cytochrome c oxidase activation), and facilitate microcirculatory improvements without imposing high mechanical stress.
- Bone marrow edema/lesions: For bone marrow edema (BME) or bone marrow lesions (BML)—conditions often linked to subchondral stress and pain—shockwave may be utilized to enhance regional perfusion and stimulate local healing responses. Timing is critical; I coordinate sessions to avoid interfering with the acute inflammatory window of PRP (typically delaying high-energy shockwave for 1–2 weeks post-injection if target tissues are adjacent and could share nociceptive pathways).
- Tendon indications: In recalcitrant tendon injuries—notably Achilles tendinopathy—pairing PRP with an appropriately dosed shockwave protocol can yield superior outcomes. Achilles tendon’s relatively robust structure, its load-bearing role, and its propensity for persistent neovascularization make it amenable to gradual mechanical stimulus. Shockwave may disrupt aberrant neovessels and nociceptive nerve ingrowth while promoting anabolism.
- Dosimetry and sequencing: I titrate energy flux density and number of pulses to match tissue tolerance, often starting at lower intensities and escalating only if pain responses remain acceptable. I avoid immediate post-PRP shockwave over the exact injection site in irritable tendons. Laser therapy serves as a bridge modality to stabilize pain and energy metabolism before shockwave introduction.
- Central sensitization considerations: For patients with widespread hyperalgesia, catastrophizing, or sleep dysregulation, I prioritize education, graded exposure, sleep hygiene, and sometimes non-pharmacologic neuromodulation strategies before adding shockwave. Mechanical overdrive in these contexts risks backfiring.
In short, shockwave is a powerful tool, but only when tissue readiness and patient neurobiology align. The pairing with PRP is diagnosis-specific, stage-specific, and calibrated to the patient’s sensory profile.
Clinical Indications and Tissue-Specific Reasoning
Orthobiologics are not one-size-fits-all. I tailor PRP composition, volume, and injection technique to the target tissue:
- Tendon Pathologies (e.g., lateral epicondylitis, patellar tendinopathy): I often favor a composition that permits a brief inflammatory response, supporting tenocyte activation and collagen remodeling. Fibroblast stimulation TypeType I collagen synthesis are central goals.
- Ligament Sprains: Similar to tendons, controlled inflammation can aid remodeling. Ultrasound guidance ensures precise delivery along ligament fibers.
- Knee Osteoarthritis: For intra-articular injections, I typically reduce granulocytes to mitigate inflammatory flares and potential chondrotoxicity. Goals include pain reduction, synovial health, and subchondral support.
- Plantar Fasciopathy: A targeted, controlled inflammatory stimulus plus mechanical unloading strategies can improve fascial integrity and pain.
- Rotator Cuff Tendinopathy: Composition aligns with tendon goals; ultrasound guidance is critical due to complex anatomy and bursae involvement.
- Post-surgical Adjuncts: Autologous biologics may support healing in selected cases, enhancing angiogenesis and matrix deposition around repair sites.
In each scenario, I consider:
- Pathophysiology: degenerative matrix, neovascularization, local cytokine milieu
- Mechanical environment: load-sharing, stress shielding, and movement patterns
- Patient factors: age, metabolic status, comorbidities, medications, platelet baseline
- Desired biologic effect: inflammation modulation, angiogenesis, matrix synthesis, nociceptive pathway impact
Detailed PRP Protocol: Step-by-Step Technique and Rationale
Device preparation:
- Anticoagulant port sterilization: I wipe the sealing port with sterile alcohol and draw up 6 mL of ACD-A into a 60 mL syringe.
- Device coating: I may gently coat the internal device surfaces with ~1 mL ACD-A to minimize microclot adherence; then I remove excess fluid.
Blood draw:
- Needle: 19-gauge butterfly for patient comfort and adequate flow.
- Volume: Up to 60 mL total, inclusive of the 6 mL ACD-A.
- Handling: Detach tubing, cap the syringe, invert ~15 times to mix anticoagulant thoroughly.
Centrifugation setup:
- Transfer: Move the filled syringe to the concentrating device.
- Caps: Place appropriate silicone and safety caps.
- Weight calibration: Using water in a counterbalance device, I ensure weight is within 1 g of the sample.
- Spin: 3500 RPM for 10 minutes (PRP 60 setting), balancing separation efficiency and platelet preservation.
Post-spin processing:
- Removal: Carefully extract the device, confirming clear separation—RBCs at bottom, buffy coat midline, PRP above.
- Benchtop station: Insert the device with the interface marking visible; the lighted version enhances interface visualization.
- Plasma advancement: Slowly twist the handle to push PPP into a primed 60 mL syringe, stopping as the buffy coat approaches the 6 mL mark.
- Buffy coat capture: Switch to a primed 12 mL syringe, dial away to capture the entire buffy coat; a slight red flash indicates entry into the interface.
Composition tuning:
- Standard PRP: For most applications, 6–7 cc is sufficient, balancing dose and viscosity.
- “Rich” style PRP: Advancing ~0.5 mL past the buffy coat increases leukocyte content for specific indications; expect a pink-to-red final hue after resuspension.
Quality checks:
- Visual: Color should be consistent with intended composition; minimal RBC contamination.
- Function: Syringe barrels must move freely to avoid pressure spikes during injection.
- Counting: I measure platelet concentration and leukocyte profile to confirm dose and composition.
Rationale:
- The exactness of interface control allows tailored leukocyte content and high platelet recovery, translating to targeted clinical effects with reduced variability.
- Single-spin design simplifies workflow, lowers error risk, and improves reproducibility in busy clinical settings.
Advanced Adjuncts: The Power of Protein Concentrate
Throughout this discussion, I’ve mentioned the use of an adjunctive therapy: an autologous protein concentrate. This is a powerful tool in my regenerative toolbox, and it’s important to understand what it is and why I use it. A patient astutely asked for clarification on whether this was a specific protein like globulin. The answer is that it’s a concentrate of many large proteins naturally found in the patient’s own blood.
The product I use is derived through a system from Apex Biologics. The process begins with the platelet-poor plasma (PPP), which is the plasma left over after we’ve harvested the buffy coat to make our PRP. Instead of discarding this PPP, we can use it to create another valuable biologic. The PPP is pushed through a specialized, pre-wetted filter with a specific pore size of fifteen kilodaltons (15 kDa).
This filter works by a process of dehydration and size exclusion. Water and small molecules pass through the filter, but large proteins (those larger than 15 kDa) are retained and become highly concentrated. The result is a smaller volume of fluid that is super-concentrated with beneficial proteins. The two most important proteins that we concentrate with this method are:
- Alpha-2-Macroglobulin (A2M): As I mentioned earlier, A2M is one of the body’s most powerful broad-spectrum protease inhibitors. In a degenerative joint or tendon, there is an overabundance of destructive enzymes called proteases, including matrix metalloproteinases (MMPs) and aggrecanases. These enzymes chew up cartilage, collagen, and other matrix proteins. By concentrating and injecting A2M, we are delivering a powerful force to trap and neutralize these destructive enzymes, shifting the joint environment from a catabolic (breaking down) state to an anabolic (building up) one.
- Interleukin-1 Receptor Antagonist Protein (IRAP): Also known as IRAP, this is the body’s natural anti-inflammatory protein that specifically targets Interleukin-1 (IL-1). IL-1 is a master pro-inflammatory cytokine that drives pain, inflammation, and cartilage degradation in conditions like osteoarthritis. IRAP works by binding to the IL-1 receptors on cells without activating them, effectively blocking IL-1 from delivering its inflammatory signal. This can significantly reduce pain and inflammation within the Joint.
I use this protein concentrate in two main ways. First, as discussed, I often co-inject it with PRP to help modulate the post-injection inflammatory flare by neutralizing MMPs and IL-1. Second, in some cases of pure osteoarthritis without significant ligamentous instability, I may use the protein concentrate as a standalone treatment. It provides a powerful anti-inflammatory and tissue-protective effect, making it an excellent option for patients who are primarily seeking pain relief and a slowing of degenerative changes. This advanced technique allows us to further customize our treatments, leveraging different components of the patient’s own blood to achieve specific biological goals.
Ethical, Compliant Growth in Orthobiologics: The Three-Legged Stool
Sustainable success in orthobiologics is not achieved through bold claims—it’s built through patient trust, regulatory compliance, and practice growth, each reinforcing the others.
- Patient trust: Without trust, patients do not proceed, refer, or become advocates. Trust stems from transparent communication, balanced discussion of benefits and limitations, realistic expectations, and follow-through. In orthobiologics, where the evidence is still evolving, humility and clarity are essential.
- Regulatory compliance: In the United States, the FDA regulates products and devices, ensuring that the biologics and tools used meet standards of safety and manufacturing quality. The FTC regulates advertising claims—what you say about those products—policing deceptive or unsupported statements. State medical boards oversee the practice of medicine and professional conduct. Understanding this multi-regulator landscape prevents missteps.
- Practice growth: Growth should be a natural outcome of trust and compliance. Evidence-driven messaging builds credibility, while procedural excellence and patient outcomes drive referrals. The ethos: aim to be the most trusted voice, not the loudest.
This framework ensures that clinical decisions are scientifically defensible and that public communications are fair, accurate, and consistent with regulatory expectations—creating a durable foundation for your practice.
Green, Yellow, Red: A Practical Risk Framework for Orthobiologics
I categorize orthobiologic applications by regulatory and evidentiary risk:
-
PRP Processing Final Product Green Zone: Autologous biologics (e.g., PRP, bone marrow concentrate) processed with FDA-compliant methods and 510(k)-cleared devices, communicated using evidence-based language. Low regulatory risk when performed to standard-of-care.
- Yellow Zone: Emerging applications or novel protocols with growing—but not definitive—evidence. Requires strong documentation, informed consent, clear rationale, and careful patient selection.
- Red Zone: Unapproved biologic products, unsupported claims (e.g., cures without evidence), or misleading advertising. The risk/reward does not make sense for physicians devoted to ethical practice.
Staying predominantly in the Green while thoughtfully engaging the Yellow empowers innovation without jeopardizing licensure or patient trust.
Autonomy, Access, and Value in a New Orthobiologics Treatment Model
Transitioning from an insurance-driven orthopedic workflow to a cash-based orthobiologics practice has been transformative to the modern treatment protocols. Historically, doctors treated many patients daily, and the default pathway often involved physical therapy, corticosteroid injections, “come back when it’s worse,” or surgery. With orthobiologics, I can serve the majority of non-surgical patients—often 75–90% of an orthopedic caseload—with proactive, regenerative care.
Why this model adds value:
- Autonomy: Free from pre-authorization delays and denials, I can tailor care to clinical need rather than payor constraints.
- Continuity: I can maintain and treat patients when they present, rather than deferring care until surgical candidacy emerges.
- Economic realism: With Medicare reimbursement reductions (e.g., ~4% cuts year-over-year) and commercial payers covering less despite higher premiums and deductibles, cash-based orthobiologics can sustain practice viability while providing transparent value to patients.
- Patient agency: Individuals choose biologic care paths aligned with their goals and timelines, supported by clear education about expected outcomes.
Ethically, this model demands:
- Transparent disclosure: Costs, expected benefit ranges, uncertainties, and alternatives (including surgery).
- Evidence alignment: Using data-driven protocols, tracking outcomes, and adjusting care based on observed efficacy and safety.
- Access considerations: Offering tiered options and discussing affordability openly, while avoiding inappropriate upselling.
Summary, Conclusion, and Key Insights
Date of Content Creation: June 11, 2026
Summary
This educational post, presented from my perspective as Dr. Jimenez, DC, FNP-APRN, provides a deep and comprehensive exploration of advanced Platelet-Rich Plasma (PRP) therapy. On June 11, 2026, I prepared this synthesis to clarify how I utilize PRP, protein concentrates, laser therapy, and shockwave therapy in musculoskeletal care with an emphasis on ethical, compliant practice growth. We challenged the old paradigm of avoiding red blood cells (RBCs) in PRP, explaining the modern rationale for including the top of the RBC layer to maximize the harvest of platelets and crucial mononuclear cells. We discussed mitigating the inflammatory flare by using autologous protein concentrates rich in A2M and IRAP.
We then detailed the importance of tailoring injectate volumes to specific joints, providing guidelines for large (knee, shoulder), medium (hip, ankle), and small (elbow, wrist, digits) joints. This led to a discussion of the “joint as an organ” concept, emphasizing a comprehensive approach that treats the entire functional joint unit. For lateral epicondylitis, PRP alone is often sufficient, supported by staged isometric-to-eccentric loading. In small joints, I use a 3:1 or 4:1 PRP-to-PC ratio; in large joints, I may employ 1:1. We also covered my detailed pre- and post-procedure protocols, reframing the inflammatory flare as a positive sign of healing and outlining a multi-modal strategy for symptom management.
A significant portion was dedicated to practice management and ethics. The shift to a cash-based model restores autonomy and continuity of care. Ethically scaling an orthobiologics practice relies on the three-legged stool of patient trust, regulatory compliance, and practice growth. The FDA governs products/devices; the FTC governs claims; state boards oversee professional conduct. I advocate the Green/Yellow/Red risk framework: prioritize autologous biologics with compliant devices, document off-label rationales robustly, and avoid unapproved products. Finally, we clarified my follow-up and redosing strategy, using the 50% improvement mark at eight weeks as a key benchmark for deciding whether a second injection is warranted.
Conclusion
The field of regenerative medicine is in a constant state of evolution, driven by modern, evidence-based research and a deeper understanding of cellular physiology. The successful application of therapies like PRP extends far beyond simply injecting a patient’s own platelets back into them. The most effective orthobiologic care marries precise tissue-specific protocols with transparent, compliant communication. By embracing concepts like cell-dosing, treating the functional joint unit, and strategically managing the inflammatory response, we can move beyond simply managing symptoms and offer our patients a genuine opportunity for true tissue regeneration and lasting functional restoration. In practice strategy, compliance is a differentiator. Being the most trusted voice, grounded in evolving evidence and ethical clarity, outperforms loud marketing in the long run. The goal is always a durable, “one-and-done” outcome, and the principles outlined here provide a robust framework for achieving that goal.
Key Insights
- Rethinking PRP Composition: Don’t fear the red. Capturing the top of the red blood cell layer is a worthwhile trade-off to secure a higher concentration of platelets and essential mononuclear cells.
- The Joint is an Organ: Effective treatment requires a comprehensive approach. Addressing extra-articular instability in ligaments and tendons is often as important, if not more so, than the intra-articular injection itself.
- Inflammation is the Goal, Not the Enemy: The acute inflammatory flare post-PRP is a sign of a successful initiation of the healing cascade. The clinical goal should be to manage symptoms and accelerate the patient through this phase, not to suppress it.
- Dose and Delivery are Paramount: Many so-called “PRP failures” are actually failures of dose or delivery. A therapeutic dose delivered with precision using ultrasound guidance is non-negotiable for predictable success.
- Rehabilitation Directs Remodeling: The biological healing stimulated by PRP is only half the battle. A structured rehabilitation program with progressive mechanical loading is the crucial signal that directs new collagen to remodel into strong, organized, and functional tissue.
- Compliance is a Competitive Advantage: Build your practice on trust, compliance, and growth; align all messaging with FDA/FTC/state board expectations to become the most trusted voice in your community.
References
- Cook, J. L., & Purdam, C. R. (Literature on tendinopathy pathology and rehabilitation models). Note: Their seminal work on the continuum model of tendinopathy and loading protocols is essential reading, often found in the British Journal of Sports Medicine.
- Evans, C. H., et al. (Fundamental research on the role of cytokines like IL-1 and growth factors in joint pathology and repair). Note: Dr. Evans is a foundational scientist in this field; his work can be found in journals like Arthritis & Rheumatism and the Journal of Orthopaedic Research.
- FDA and FTC public guidance documents on medical devices and advertising claims.
- Interventional Orthobiologics Foundation. Clinical and research resources on orthobiologics.
- Biologics Association. Standards and consensus statements in biologics.
- LaPrade, R. F., et al. (Studies on the “functional joint unit” and the importance of ligamentous structures). Note: Research from Dr. LaPrade’s group often appears in the American Journal of Sports Medicine and Arthroscopy.
- Mautner, K., et al. (Research on PRP composition, leukocyte concentration, and clinical outcomes). Note: Dr. Mautner has published extensively on orthobiologics. Search for his work in journals like PM&R and the Clinical Journal of Sport Medicine.
- Peer-reviewed literature on PRP compositions, growth factor kinetics, and clinical outcomes in musculoskeletal indications.
- Peer-reviewed literature on PRP efficacy in tendinopathy, tendon remodeling mechanisms, photobiomodulation effects, and shockwave therapy indications and dosing.
- Podesta, L., et al. (Literature on PRP dose-dependency for lateral epicondylitis). Note: Specific papers by Luca Podesta and colleagues on this topic can be found in journals such as the American Journal of Sports Medicine or PM&R.
- (Research on the chondrotoxicity of local anesthetics). Note: Numerous studies on this topic can be found in journals such as Arthroscopy and the Journal of Bone and Joint Surgery.
- (Research on Autologous Protein Concentrates, A2M, and IRAP). Note: Search for these terms in orthopedic and sports medicine journals for studies on their mechanism and clinical application.
- Clinical consensus statements and best-practice guidelines for musculoskeletal injections and regenerative protocols.
- Clinic hemocytometer data and internal quality assurance protocols for PRP dose and recovery tracking.
Disclaimer: The information provided in this educational post is for informational purposes only and is not intended to be a substitute for professional medical advice, diagnosis, or treatment. This content reflects the clinical experience and knowledge of Dr. Jimenez, DC, FNP-APRN, as of the content creation date (June 11, 2026), and is based on evidence and practices that are constantly evolving. It should not be used as a personal medical guide.
Disclaimer for Individual Medical Advice: All individuals are unique, and medical conditions vary. You must consult with your own qualified medical provider for any health concerns or before making any decisions related to your health or treatment. The protocols and opinions expressed in this post are generalized and may not be appropriate for your specific situation. Do not disregard, avoid, or delay obtaining medical advice from a qualified healthcare professional because of something you have read here. Reliance on any information provided in this post is solely at your own risk.
Post Disclaimer
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Advanced PRP Science, Autologous Therapies, and Updated Practice Innovations" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine; wellness; contributing etiological viscerosomatic disturbances within clinical presentations; associated somato-visceral reflex clinical dynamics; subluxation complexes; sensitive health issues; and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and licensure jurisdiction. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that directly or indirectly relate to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
New Mexico CNP License#: 90560, Verified
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
| Yes | 363LF0000X - Nurse Practitioner - Family | NM |
90560 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
📆 Schedule Appointment: Schedule 24/7 (Click Here)