


Table of Contents
Abstract
In this educational post, I will walk you through how I approach a complex spine and neuroinflammatory case in clinical practice, integrating traditional, functional, and advanced regenerative medicine. My goal is to show how modern, evidence-based concepts from leading researchers can be applied in a structured, clinically meaningful way.
We begin with a common clinical scenario: a patient with chronic neck and low back pain, possible facet joint dysfunction, discogenic pain, or nerve irritation—the type of case most clinicians see every day. In a conventional framework, we might stop at structural diagnoses: disc pathology, facet arthropathy, or nerve trauma. However, modern research consistently shows that this picture is often incomplete. Chronic pain and degeneration are frequently intertwined with neuroinflammation, toxin burden, immune dysregulation, and systemic metabolic stress.
I will then expand the lens to a functional medicine perspective, asking not only what hurts and where, but also why the system is inflamed and dysregulated. We will examine how chronic liver inflammation, lymphatic congestion, cardiometabolic dysfunction, gut dysbiosis, and impaired glymphatic (brain lymphatic) drainage create a milieu of brain inflammation, microcirculatory stagnation, immune disruption, and toxic accumulation. These upstream drivers may be the key to resolving what appears to be purely musculoskeletal.
From there, I will detail how postural biomechanics, particularly forward head posture and connective tissue laxity, can drive cervical instability, vagus nerve dysfunction, TMJ pain, tinnitus, vertigo, and autonomic dysregulation. We will look at how mechanical stress on the cranio-cervical junction, carotid and vertebral arteries, and upper cervical spinal cord can translate into systemic symptoms via hypoxia, dysautonomia, and persistent nociceptive input.
Next, I outline a realistic diagnostic workflow: from standard imaging (MRI, ultrasound) and laboratory studies to advanced functional assessments (gut microbiome, inflammatory markers, toxin panels, nutrient status, mitochondrial function). The goal is to build a holistic yet mechanistically coherent model of the patient’s condition, rather than a disconnected list of findings.
Once we establish a comprehensive picture, we move into strategic treatment layering. First, we prepare the terrain: reducing inflammatory burden, addressing sterile vs. non-sterile inflammation, optimizing mitochondrial function, stabilizing the neuroendocrine axis, and improving gut and detoxification pathways. Only then do we apply precision regenerative interventions, such as facet joint injections, exosomes, and, in select cases, novel pluripotent-like cell therapies (e.g., Muse cells – multilineage-differentiating stress-enduring cells), based on emerging research from Japan and other leading centers.
A significant portion of this post delves into the biology of inflammation and cellular senescence—including PAMPs and DAMPs, sterile vs. non-sterile inflammation, and the difference between early P21-type senescence and chronic P16-dominant senescence (so-called “zombie cells”). I will explain why this matters for pain, degeneration, and regenerative success, and how specific interventions—nutritional, pharmacologic, and peptide-based—are selected.
I also discuss peptides and biologic therapeutics, emphasizing the critical importance of purity, manufacturing methods, regulatory oversight, and quality control. We’ll review how peptides are produced (solid-phase synthesis and vector-based production) and why this matters for patient safety in sensitive patients.
Finally, I present clinical cases involving new cell-based therapies (Muse-type cells and exosomes) in spinal and shoulder pathology, highlighting real imaging outcomes, clinical responses, and plausible mechanisms. We close with recovery and optimization strategies, then summarize the major key insights for clinicians and patients.
Evidence-Based Spine & Neuroinflammation Care: My Clinical Framework
From Traditional Spine Diagnosis to Systems-Level Thinking
When a patient presents to my clinic with neck or low back pain, my initial mental checklist looks similar to most traditional approaches:
- Disc pain (disc herniation, disc degeneration, annular tears)
- Facet joint pain (facet arthropathy, capsular strain, inflammatory synovitis)
- Nerve trauma or irritation (radiculopathy, nerve root compression, dorsal root irritation)
In a purely structural model, this triad often defines the diagnosis: disc, facet, or nerve. Standard workup might include:
- MRI to evaluate discs, joints, nerves, and bone marrow edema
- Ultrasound for dynamic or soft-tissue assessment (e.g., tendons, ligaments)
- Basic labs for inflammation (e.g., CRP, ESR), metabolic status, and sometimes rheumatologic screening
However, in practice, and supported by current literature, it becomes clear that these “local” pathologies are often embedded in a broader systemic context. Many patients do not respond predictably to interventions targeting only the spine. When I see this mismatch, I immediately consider functional and systemic factors.
Functional Medicine Perspective: Neuroinflammation, Toxins & Systemic Stress
 Beyond the Disc: Neuroinflammation and Toxin Burden
Beyond the Disc: Neuroinflammation and Toxin Burden
From a functional medicine vantage point, I ask: What else could be driving or amplifying this pain? Some key domains include:
- Chronic liver inflammation
- Lymphatic dysfunction and impaired drainage
- Cardiometabolic dysfunction (“cardiopathy” in a broader functional sense)
- Gut-derived inflammation (dysbiosis, leaky gut, endotoxemia)
- Brain glymphatic impairment (impaired clearance of metabolic waste)
- Toxin accumulation (mold, heavy metals, environmental xenobiotics)
- Chronic low-grade infections (viral reactivation, biofilm-associated bacteria, oral/sinus pathogens)
Each of these systems interfaces with neuroinflammation, often via:
- Microglial activation
- Cytokine signaling (e.g., IL-1β, IL-6, TNF-α)
- Blood–brain barrier (BBB) permeability
- Vagal and autonomic imbalance
If the brain’s waste clearance (glymphatic/lymphatic outflow) is impaired, metabolic byproducts and inflammatory mediators accumulate, leading to chronic brain inflammation and microcirculatory stagnation. Clinically, this can manifest as:
- Brain fog
- Headache
- Central pain amplification
- Autonomic dysregulation (e.g., POTS-like symptoms, orthostatic intolerance)
When a spine patient also exhibits cognitive, mood, or autonomic issues, this systemic angle becomes essential.
Posture, Cervical Instability & Autonomic Dysfunction
Forward Head Posture and Connective Tissue Disorders
One of the most underestimated contributors I see is chronic forward head posture, combined with connective tissue laxity (hypermobile syndromes, collagen disorders).
As the head drifts forward, several things happen:
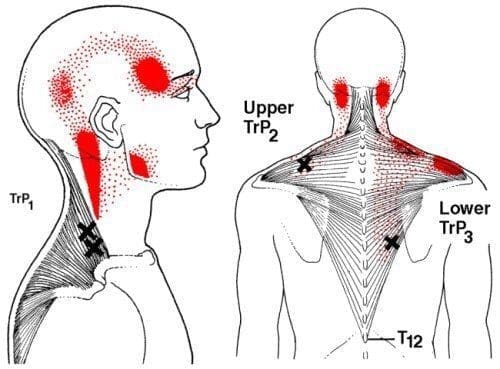
- The cervical extensor musculature must work harder to hold the head up, leading to overuse and myofascial trigger points.
- The facet joints and capsular ligaments of the cervical spine—especially the upper cervical and craniocervical junction—experience chronic tensile stress.
- In patients with connective tissue disorders (e.g., hypermobility, EDS spectrum), these capsular ligaments can become stretched, leading to segmental instability.
Over time, this can result in:
- Cervical instability
- Facet capsule strain
- Sacroiliac and pelvic ligament strain, as the entire kinetic chain compensates
Cervical Instability and Vagus Nerve & TMJ-Related Symptoms
 With cervical instability, especially at C0–C2, I often see:
With cervical instability, especially at C0–C2, I often see:
- Vagus nerve dysfunction:
- The vagus nerve emerges from the jugular foramen and travels near upper cervical structures.
- Chronic mechanical irritation or congestion can impact vagal tone, affecting heart rate, digestion, inflammatory modulation, and mood.
- TMJ pain:
- Forward head posture alters mandibular position and occlusal alignment, thereby overloading TMJ structures.
- Cervical proprioception and jaw mechanics are tightly integrated via the trigeminal system and cervical afferents.
- Tinnitus and vertigo:
- Upper cervical dysfunction can affect vertebral artery flow, inner ear circulation, vestibular nuclei via, altered sensory input, and microvascular changes.
- Chronic neuroinflammation around the brainstem and cerebellum further aggravates these symptoms.
Mechanical Compression of Vessels and Neural Structures
As the head moves forward and the neck becomes unstable:
- There may be mechanical compression or kinking of the carotid and vertebral arteries.
- This can lead to intermittent hypoxic injury of brain tissue or the cervical spinal cord, especially in certain positions.
- The upper cervical spine can encroach on the spinal cord, brainstem, and autonomic pathways.
Clinically, this can present as:
- Transient neurologic symptoms (e.g., visual disturbance, dizziness, imbalance)
- Worsening with certain head positions
- Fatigue, cognitive slowing, or “crashes” after mild exertion
All of these are common in patients who are told they have “just a bad neck” but clearly have a more systemic problem.
Diagnostic Strategy: From Imaging to Systems Evaluation
Standard Imaging and Laboratory Evaluation
After a thorough physical and neurologic examination, I typically begin with:
- MRI (cervical, thoracic, lumbar as indicated)
- Disc integrity
- Facet joint degeneration
- Bone marrow edema (Modic changes)
- Spinal canal and foraminal stenosis
- Ultrasound (for certain joints and soft tissues)
- Diagnostic blocks or guided injections (when appropriate to confirm pain generators)
Basic labs may include:
- Complete blood count (CBC)
- Comprehensive metabolic panel (CMP)
- Inflammatory markers: CRP, ESR
- Lipid profile, glucose, HbA1c
- Thyroid function
Advanced Functional Testing
When the presentation suggests a broader systemic process, I layer in additional testing:
- Gut microbiome and dysbiosis panels
- Evaluating bacterial diversity, pathobionts, short-chain fatty acid production, and yeast overgrowth
- Assessing leaky gut (e.g., zonulin, LPS) when indicated
- Oral and sinus microbiome/infection assessment
- Periodontal disease, root canal infections, cavitations
- Chronic sinus colonization with biofilms
- Toxin burden
- Mold mycotoxins
- Heavy metals
- Environmental pollutant profiles (when clinically indicated)
- Nutrient markers
- Vitamins (e.g., B12, D, folate)
- Minerals (magnesium, zinc, copper, etc.)
- Amino acids, fatty acids
- Mitochondrial function tests (where available)
- Markers of oxidative stress
- Organic acids
- Hormonal and neuroendocrine evaluation
- Cortisol rhythm
- Sex hormones
- Thyroid, insulin, leptin
My objective is to identify all converging factors that might be sustaining neuroinflammation, poor tissue healing, and pain sensitization.
Building a Holistic Patient Profile
Structural, Autonomic, and Inflammatory Components
Let’s imagine we compile all this data and arrive at a working profile:
- Structural findings:
- Cervical facet arthropathy
- Myofascial restriction in the neck and upper back
- Possible disc degeneration or Modic changes
- Autonomic and central sensitization:
- Autonomic dysfunction (e.g., variable HR, POTS-like symptoms)
- Central sensitization and heightened pain response
- Sleep disturbances, difficulty modulating stress
- Inflammatory and immune components:
- Ongoing low-grade inflammation (elevated CRP or subtle immune markers)
- Possible gut dysbiosis and/or chronic infection
- Mild toxin or mold burden
When I see this pattern, I know that treating only the spine—as though it is isolated—will likely yield suboptimal results. We must treat the terrain.
Precision Interventions: Cervical Facet Injections & Regenerative Methods
Facet Joint Injections as Structural Reset Points
In a patient with significant facet joint pain, I may perform:
- Cervical facet joint injections (often under fluoroscopic or ultrasound guidance)
- Local anesthetic and, when appropriate, regenerative biologics (e.g., PRP, exosomes, or in selected contexts, advanced cell-based products depending on regulatory allowances)
- Addressing facet capsule inflammation, improving joint mechanics, and reducing nociceptive input
The intent is to:
- Interrupt chronic pain circuitry
- Reduce local inflammatory mediators
- Provide a window of opportunity for rehabilitation, postural correction, and systemic optimization.
However, I rarely consider this the “final treatment” in complex cases. It is one piece of a larger protocol.
Pre-Treatment Terrain Optimization: Why It Matters
The Role of Peptides and Preconditioning
Before any advanced regenerative intervention, I focus on “setting the terrain”—a concept that recurs frequently in modern regenerative research. This includes:
- Reducing inflammatory burden
- Optimizing nutrient status
- Supporting mitochondrial function
- Stabilizing neuroendocrine and autonomic systems
- Enhancing detox and gut function
This is where peptides and targeted nutraceuticals often come in.
Core Domains I Evaluate Before Regeneration
Before a major regenerative procedure, I systematically consider:
- Inflammation
- Is it primarily sterile or non-sterile (infectious)?
- Are we dealing with chronic senescent-cell-driven inflammation?
- Are there signs of excessive oxidative stress?
- Nutrient and substrate availability
- Are the basic building blocks for tissue repair (amino acids, micronutrients, essential fatty acids) present?
- Hormones & neuroendocrine status
- Is cortisol dysregulated?
- Are thyroid and sex hormones adequate to support regeneration and mitochondrial function?
- Mitochondrial health
- Can the cell generate enough ATP and manage reactive oxygen species (ROS) for proper healing?
- Autonomic nervous system balance
- Is there excessive sympathetic “fight or flight” dominance preventing repair?
- Detoxification and gut health
- Is the gut sufficiently functional to absorb nutrients and excrete toxins?
- Are mold or metal burdens impairing recovery?
Only after I address these factors do I feel confident that the patient’s biology is ready to respond optimally to regenerative therapy.
Inflammation 2.0: Sterile vs. Non-Sterile and Why It Matters
Non-Sterile Inflammation: PAMPs and Infection-Driven Signals
Non-sterile inflammation is driven by pathogen-associated molecular patterns (PAMPs)—specific molecular features found on:
- Bacteria
- Viruses
- Fungi
- Parasites
These molecules activate pattern recognition receptors(e.g., Toll-like receptors) on immune cells, leading to:
- Cytokine release
- Recruitment of additional immune cells
- Local tissue damage if uncontrolled
Clinical implications:
- Persistent infections (e.g., chronic sinusitis, periodontal disease, latent viral reactivation) can drive ongoing neuroinflammation and pain sensitization.
- If we misinterpret infection-driven inflammation as purely sterile inflammation and fail to treat the infectious source, regenerative therapies may underperform or fail.
Sterile Inflammation: Damage, Metabolism, and Senescence
Sterile inflammation arises in the absence of an active microbe. Instead, it is triggered by:
- Damage-associated molecular patterns (DAMPs) are released from injured or stressed cells
- Metabolic dysregulation (e.g., advanced glycation end-products, excess lipids)
- Cellular senescence (senescent cells releasing inflammatory mediators – the SASP, senescence-associated secretory phenotype)
Here, the immune system is responding to endogenous danger signals, not infectious agents.
Clinical implications:
- Chronic sterile inflammation underlies many degenerative and age-related conditions: osteoarthritis, disc degeneration, atherosclerosis, etc.
- Overzealous suppression of sterile inflammation (e.g., with NSAIDs) immediately post-injury can sometimes impair the normal healing cascade, which requires a physiologic inflammatory phase.
Cellular Senescence: P21 vs. P16 and “Zombie Cells”
Why Senescent Cells Matter in Regeneration
Cellular senescence is a state where cells stop dividing but remain metabolically active. They can secrete:
- Cytokines
- Chemokines
- Proteases
- Other factors that contribute to the inflammatory milieu (SASP)
Importantly, not all senescence is bad; some is protective and necessary during development, tissue remodeling, and acute wound healing.
P21-Dominant Early Senescence: Protective & Transient
P21-associated senescence often represents:
- Early, transient senescence
- A controlled response to stress or injury
- A signal for the body: “I’m weakened; I need support; control proliferation here.”
These cells can:
- Be cleared by the immune system once their job is done
- Play a role in orchestrating proper wound healing and regeneration
In many cases, we do not want to aggressively eliminate these cells, especially in the acute healing phase.
P16-Dominant Late Senescence: Pathologic “Zombie Cells”
P16-dominant senescence is:
- Persistent, chronic, and often pathologic
- Less likely to be cleared naturally
- More likely to produce a persistent SASP profile that drives sterile inflammation
These are the “zombie cells” that accumulate with age and chronic stress, contributing to:
- Degenerative disc disease
- Osteoarthritis
- Cardiometabolic disease
- Neurodegeneration
From a regenerative standpoint, P16-dominant senescent cells are often targets for senolytic strategies, either nutraceutical or pharmacologic, to improve the tissue environment before or alongside regenerative therapies.
Fighting Inflammation Naturally *Chiropractic Care*-Video
Preparation Goals Before Regenerative Therapy
Reducing Inflammatory Burden
I typically start by reducing systemic and local inflammatory load:
- Diet: Anti-inflammatory patterns (e.g., Mediterranean-style, low in ultra-processed foods)
- Nutraceuticals (e.g., omega-3s, polyphenols)
- Targeted interventions to lower sterile and, where appropriate, non-sterile inflammation
Some of the nutrient-based supports I might consider:
- Alpha-lipoic acid
- Vitamin D
- B-complex vitamins
- Curcumin, resveratrol, and others, as indicated
Mitochondrial Enhancement: Why It’s Central
Regeneration is ATP-intensive. Damaged tissues require:
- Energy for cell division, matrix remodeling, and ion balance
- Mitochondrial resiliency to handle increased metabolic load
I might use:
- CoQ10– supports electron transport chain function
- L-carnitine– assists in fatty acid transport into mitochondria
- N-acetylcysteine (NAC) or glutathione support– addresses oxidative stress
- Specialized peptides such as SS-31 (elamipretide, a mitochondrial-targeted peptide) in appropriate contexts
Immune Rebalancing and Neuroendocrine Stabilization
I also aim to:
- Rebalance immune function, not simply “stimulate” or “suppress.”
- Improve sleep, stress resilience, and HPA axis function
- Support vagal tone and autonomic balance (breathing exercises, HRV training, targeted supplements/peptides)
This sets the stage for better regenerative outcomes and fewer adverse responses.
Peptides: Powerful Tools, Critical Quality Concerns
Why Peptides and Why Quality Matters
In my practice, we see a significant number of sensitive patients—those with:
- Cell danger response patterns
- Multiple medication sensitivities
- Mast cell activation tendencies
- Chronic fatigue, dysautonomia, and complex multisystem illness
For these individuals, solvents, impurities, or degraded products can trigger significant reactions. This is why I am extremely cautious with peptide sourcing.
Manufacturing and Regulatory Gaps
Currently:
- Many peptides are produced overseas and then shipped into the U.S.
- Compounding pharmacies may receive bulk material and provide a certificate of analysis, but this often relies heavily on the supplier’s documentation rather than independent verification.
- Because many peptides operate in a regulatory gray zone, they can escape stringent oversight.
Potential issues include:
- Identity: Is it actually the peptide it claims to be?
- Purity: Are there contaminants, side products, or incorrect amino acid sequences?
- Potency: Does the stated dose match the actual active content?
- Sterility & endotoxin levels (for injectables)
- Stability: Has it degraded during storage or transport?
For highly reactive or fragile patients, these details are not trivial; they can make the difference between a helpful therapy and a flare.
How Peptides Are Made: Solid Phase and Vector-Based Methods
 Solid-Phase Peptide Synthesis (SPPS)
Solid-Phase Peptide Synthesis (SPPS)
One common method is solid-phase peptide synthesis:
- The first amino acid is anchored to an inert resin.
- The manufacturing system then cycles through:
- Deprotecting the terminal group
- Adding the next activated amino acid
- Washing and repeating until the full sequence is built.
SPPS is:
- Reliable and highly controlled for shorter peptides(often ≤ 15 amino acids).
- As chain length increases, the risk of incomplete coupling, misfolding, and side reactions rises, making quality control increasingly important.
Vector-Based (e.g., Yeast/Plasmid) Peptide Production
Another advanced approach involves vector-based expression:
- A plasmid carrying the peptide’s genetic blueprint is introduced into a host organism, such as yeast.
- The yeast integrates or maintains this plasmid and begins producing the peptides as it grows.
- The peptide is then isolated and purified from the culture medium.
- Quality is confirmed using tools such as mass spectrometry and HPLC (high-performance liquid chromatography).
This method can be particularly useful for:
- Complex peptides
- Longer chains
- Situations where a more “biologic-like” production system is desired
Regardless of method, I strongly emphasize:
- FDA-registered, cGMP-compliant facilities
- Third-party testing
- Transparent certificates of analysis
When I apply intensive effort to optimizing a patient’s system, I cannot afford unreliable inputs at the final therapeutic step.
Introducing Muse Cells: Multilineage-Differentiating Stress-Enduring Cells
What Are Muse Cells?
Muse cells (Multilineage-differentiating Stress-Enduring cells) represent a relatively recent discovery in regenerative medicine, with much pioneering work coming from Japanese researchers and others.
Key points:
- Muse cells reside in adult tissues, including:
- Bone marrow
- Adipose tissue
- Connective tissue and mesenchymal stromal cell (MSC) populations
- They are pluripotent-like—capable of differentiating into cell types from all three germ layers—yet do not behave like classic embryonic stem cells or induced pluripotent stem cells in terms of tumor risk.
- They are stress-enduring: they are activated and mobilized under stressful or damaging conditions (ischemia, injury, inflammation).
Before Muse cells were characterized, it was widely held that adult humans had only multipotent stem cells (e.g., MSCs) and lacked significant true pluripotency outside embryonic contexts. Muse cells challenge and refine that paradigm.
Key Biological Markers and Characteristics
Muse cells:
- Express pluripotency markers (e.g., NANOG, among others)
- Have telomerase activity, enabling extended replicative capacity
- Divide slowly, and are not hyperproliferative like typical cancer cells
- They are non-tumorigenic in experimental models, even when transplanted
In vivo, their job is to:
- Remain quiescent (like a reserve force) in tissues such as bone marrow and connective tissue
- Be mobilized under significant stress or tissue damage
- Home to sites of injury and differentiates into needed cell types, contributing to true tissue repair and regeneration
Mechanism of Action: Homing, Differentiation, and Tissue Integration
Homing via Sphingosine-1-Phosphate (S1P) and Related Signals
When tissue injury occurs—such as myocardial infarction, stroke, or severe local damage—injured cells release various signals, including sphingosine-1-phosphate (S1P).
Key points:
- S1P creates a gradient that guides certain cells (including Muse cells) to regions of injury.
- Muse cells express S1P receptors, enabling them to sense and migrate along this gradient.
- Similar homing patterns are also observed in monocytes and macrophages, but Muse cells confer a pluripotent-like regenerative capability at the site.
Differentiation and Replacement of Damaged Cells
Once at the injury site, Muse cells:
- Engraft into the damaged tissue
- Sense local epigenetic and microenvironmental cues
- Begin to differentiate into the local cell type (e.g., cardiomyocytes in the heart, neurons or glia in the brain, etc.)
Experimental models show:
- Muse cells in a damaged myocardium can adopt cardiomyocyte phenotypes and contribute to improved ejection fraction and structural repair.
- Muse cells in CNS injury models can differentiate into neural-lineage cells and support functional recovery.
To visualize this, researchers have:
- Tagged Muse cells with reporter genes (e.g., fluorescent or luminescent markers).
- Observed them initially as quiescent cells at the injury site
- Then, they noted the activation of lineage-specific genes and reported that once they commit to a particular fate (e.g., cardiomyocyte markers in heart tissue).
Immune Modulation and HLA-G Expression: Allogeneic Use
Why Muse Cells May Be Used Across Donors
One of the breakthroughs with Muse cells is their immune-modulatory profile, particularly their expression of HLA-G:
- HLA-G is a tolerogenic MHC molecule also associated with fetal-maternal tolerance in pregnancy.
- Its presence helps signal to the immune system that the cell is an “ally” and should not be aggressively attacked.
This confers several advantages:
- Muse cells can often be used in an allogeneic setting (donor-to-recipient) with minimal rejection.
- They tend to promote T regulatory (Treg) differentiation, reduce T cell proliferation, and decrease dendritic cell activation.
This implies:
- Reduced need for heavy immunosuppression compared to many other forms of cell transplantation.
- The potential for off-the-shelf Muse cell therapies in various conditions, including stroke, myocardial infarction, and neurodegenerative diseases, is pending ongoing trial outcomes and regulatory pathways.
Clinical Trials and Evidence: Stroke, Cardiac, ALS, Neonatal
Stroke
One key Japanese trial:
- Included patients with severe stroke, receiving Muse cells or a placebo.
- The Muse cell group received an intravenous dose (e.g., 25 million cells; exact dosing varies by protocol).
- Primary endpoint: improvement in modified Rankin Scale (mRS) to a defined functional level.
Reported results:
- Around 40% of Muse-treated patients achieved the endpoint, vs. about 10% in the placebo group.
- This indicates a meaningful functional recovery advantage in a severely affected population.
Heart Failure / Post-MI
In another study:
- Patients with post-MI reduced ejection fraction (EF) (e.g., <45%) received Muse cell therapy.
- Over about 35 days, EF improved from roughly 40.7% to 52% on average.
- No major safety signals emerged in these early-phase studies.
While not large, these studies are suggestive and have spurred ongoing research.
ALS and Neurologic Disease
In small pilot cohorts:
- Muse cells have been administered to patients with ALS.
- In one report of 5 patients, 4 appeared to stabilize for a time, while one continued to progress.
These are early data, not definitive, but they highlight a potential role in neurodegenerative conditions.
Neonatal and Pediatric Populations
Muse cells have also been tested in:
- Neonates with certain forms of brain injury or risk (e.g., hypoxic-ischemic injury).
- Small trials (e.g., involving about nine neonates) have suggested safety and possible benefit, though these populations require extreme caution and long-term follow-up.
Collectively, these data support Muse cells as a promising, emerging modality with a significant research base, particularly from Japan, and growing interest worldwide.
Why Not Just Use Bone Marrow MSCs? Muse Cell Purity and Competition
Muse vs. Conventional MSC Preparations
Muse cells make up roughly 1–3% of the cells in bone marrow and some MSC preparations. That leads to a logical question:
“Can I just take bone marrow, inject it, and count on the Muse cells within it to do the job?”
Research suggests:
- When standard MSC mixtures (containing both Muse and non-Muse cells) are injected, non-Muse MSCs tend to dominate the local environment.
- These non-Muse cells might secrete signals that inhibit or overshadow the regenerative actions of Muse cells.
- As a result, only a small fraction of Muse cells may reach the injury site and effectively participate in regeneration.
Importance of Muse Cell Enrichment
Data indicate that:
- You may need ≥70–75% Muse cell purity to achieve the full regenerative benefits observed in controlled experimental models.
- When researchers compared fluorescent tracking of Muse-enriched vs. non-Muse cells, they observed that Muse cells homed to and integrated into the target tissue. In contrast, non-Muse cells showed minimal, durable presence.
Thus, advanced enrichment and isolation techniques are essential if we wish to replicate the true Muse cell effect seen in preclinical studies.
Clinical Application: Musculoskeletal and Spine Cases
Case 1: Lumbar Disc Collapse with Bone Marrow Edema – Exosome-Based Strategy
Patient: Male, mid-30s
History:
- Developed significant low back pain after receiving a vaccine (temporal association).
- Persistent pain with sitting and standing, worsened by flexion and extension.
Imaging:
- MRI showed an L1–L2 disc essentially collapsed.
- Adjacent vertebral bodies exhibited marrow edema (a form of Modic change), indicating ongoing inflammatory activity in the bone.
Intervention:
- I chose to use exosomes(cell-free vesicles derived from Muse or MSC populations) rather than injecting Muse cells directly into the epidural space.
- Rationale:
- At the time, safety data for direct epidural Muse cell injections were limited.
- The epidural space is relatively open and free-flowing; I prefer caution until more robust data exist.
- Administered 100 million exosome units via epidural injection at the affected level.
Outcome:
- Follow-up MRI showed resolution of the marrow edema.
- The collapsed disc did not regrow (as expected), but the patient’s pain significantly improved, and functional capacity increased.
Physiologic reasoning:
- Exosomes deliver regenerative and anti-inflammatory signals without the cells themselves.
- They can modulate local immune cells, endothelial function, and possibly stimulate resident progenitor cells.
- By calming bone marrow inflammation and possibly altering the local microenvironment, pain and function improved even without structural disc restoration.
Case 2: Shoulder Injection with Muse Cells and Exosomes; Unexpected Lumbar Effect
Patient: Female, mid-40s
Presenting complaint:
- Left shoulder pain, diagnosed as a supraspinatus tear.
- During history-taking, she also reported axial low back pain, but our immediate focus remained on the shoulder.
Intervention (Shoulder):
- Injected 20 million Muse cells into the shoulder region, combined with exosomes.
- Imaging guidance is used to ensure precise placement within and around the supraspinatus tendon and associated structures.
Post-treatment course:
- Shortly after treatment, she experienced a flare of her low back pain.
- She obtained a lumbar MRI, which revealed increased fluid/effusion in the facet joints—suggestive of a transient inflammatory or dynamic response.
Subsequent evolution:
- Over the next several days, she reported significant improvement in her low back symptoms, beyond baseline.
Interpretation:
- A plausible explanation is that some of the systemically circulating Muse cells and/or exosomes homed to the previously inflamed lumbar facet joints, transiently altering local fluid dynamics and inflammation.
- The effusion may represent an acute phase of regenerative remodeling.
- As inflammation resolved and tissue normalized, the patient experienced reduced pain and improved function.
Key insight:
- Muse cells’ ability to home to distant sites of injury—even when initially injected locally—can sometimes produce far-reaching clinical effects.
- This has implications for systemic vs. local administration strategies in future clinical protocols.
Safety, Complications, and Future Directions
Observed Side Effects
Muse cells and related regenerative injections share some general risk patterns with other interventional procedures:
- Mild:
- Low-grade headache
- Fatigue or transient flu-like symptoms
- Local soreness or temporary symptom exacerbation
- Severe (rare but possible with any invasive procedure):
- Infection
- Vascular complication or bleeding
- Neurologic injury if the anatomy is not meticulously respected
In my own experience, major complications have been extremely rare; nonetheless, they are always considered and addressed in the informed consent process.
Timing of Muse Cell Administration After Injury
A frequent question is:
“When is the best time to administer Muse cells after an acute injury—early or delayed?”
Based on existing trials:
- The stroke trial often administered Muse cells in the 3–5 day window post-event.
- This window appears to allow initial inflammatory and clean-up processes to begin, while still providing substantial regenerative benefit.
Conceptually:
- In younger patients with robust endogenous Muse and stem cell responses, immediate administration might be less critical, or timing may be more flexible.
- In older patients, whose endogenous regenerative capacity is diminished, earlier therapeutic support may be more important.
We still do not have definitive answers; ongoing and future trials will refine:
- Optimal dosing
- Optimal timing
- Optimal route of administration(IV, local injection, intranasal, etc.)
Recovery and Optimization After Regenerative Treatments
 Post-Procedure Goals
Post-Procedure Goals
After regenerative interventions (e.g., Muse cells, exosomes, PRP, advanced facet injections), my focus shifts to:
- Accelerating tissue repair and angiogenesis
- Maintaining sufficient, but not excessive, inflammation for healing
- Protecting mitochondria during the high-energy phase of regeneration
- Optimizing biomechanics and neuromuscular control
I strongly advise:
- Avoiding NSAIDs in the crucial post-procedure window, as they can blunt the natural inflammatory phase needed for tissue remodeling.
- Carefully titrating activity: avoiding both extreme immobilization and premature overuse.
Peptides and Mitochondrial Support in Recovery
Common peptide and nutrient tools may include:
- BPC-157– often used for gut and musculoskeletal healing support
- TB-500 (thymosin beta-4)– involved in actin dynamics, tissue repair (used cautiously and in appropriate contexts)
- GHK-Cu– copper-binding tripeptide with roles in tissue repair and anti-inflammatory modulation
- Mitochondrial supports: CoQ10, acetyl-L-carnitine, NAC, and others
These are selected individually, based on:
- Patient sensitivity
- Specific tissue and systemic needs
- Regulatory status and evidence base
Lifestyle, Sleep, and Rehabilitation
Recovery is not only biochemical:
- Sleep: deep, restorative sleep is one of the most potent regenerative forces.
- Nutrition: adequate protein, micronutrients, and healthy fats are essential for tissue building.
- Postural and movement rehabilitation: re-training cervical alignment, pelvic stability, and core control is vital to ensure that newly repaired tissues are not immediately re-damaged by poor biomechanics.
In essence, the regenerative treatment is a catalyst, not a standalone cure. The patient’s daily environment, stressors, and movement patterns must be aligned with healing.
Summary
Summary
This educational post outlines how I, as a clinician with training in chiropractic and advanced nursing practice, integrate traditional, functional, and regenerative medicine to treat complex spine and neuroinflammatory conditions in a modern, evidence-based manner.
We began with a typical spine case—chronic neck or low back pain—where a strictly structural approach focuses on discs, facet joints, and nerve irritation. While this remains essential, it is often insufficient to explain or resolve the patient’s condition fully. Accordingly, I broaden the lens to consider systemic drivers: neuroinflammation, toxin burden, gut dysbiosis, lymphatic and glymphatic dysfunction, and immune dysregulation.
We then examined the impact of postural biomechanics, especially forward head posture and connective tissue laxity, on cervical instability, vagus nerve dysfunction, TMJ pain, tinnitus, vertigo, and autonomic imbalance. These mechanical stresses can compress vascular and neural structures, leading to hypoxia and persistent nociception, which feed back into central sensitization.
The diagnostic strategy follows a layered approach: standard tools such as MRI, ultrasound, and basic labs are augmented by functional assessments of the gut microbiome, oral/sinus health, toxins, nutrients, mitochondrial function, and hormonal status. The goal is to construct an integrated model that connects structural findings to systemic context.
We then moved into terrain preparation, emphasizing why regenerative treatments should not be deployed into a hostile biological environment. I discussed sterile vs. non-sterile inflammation—the former driven by endogenous danger signals and senescence, the latter by pathogens and PAMPs. Understanding this distinction is key when choosing between antimicrobial, anti-inflammatory, senolytic, or tolerance-promoting strategies.
The concept of cellular senescence—particularly the difference between P21-dominant early senescence and P16-dominant chronic “zombie” senescence—helps clarify when the body’s response is adaptive and when it becomes pathologic. This informs the timing and intensity of interventions aimed at clearing senescent cells or modulating their secretory profile.
We examined peptides as powerful, targeted tools but highlighted their dependence on high-quality manufacturing, purity, and stability, particularly in sensitive patients. I described key production methods—solid-phase synthesis and vector-based expression—to underscore why rigorous cGMP production and third-party testing are non-negotiable in my practice.
A major section addressed Muse cells (multilineage-differentiating stress-enduring cells), including their origin, characteristics, and unique properties:
- Pluripotent-like capabilities without typical tumor risks
- Residence in adult tissues (bone marrow, adipose, connective tissue)
- Stress-induced mobilization and homing to injury sites via signals like S1P
- Differentiation into local cell types (e.g., cardiomyocytes, neural cells)
- Expression of HLA-G, which supports immune tolerance and enables promising allogeneic use
I reviewed early clinical data in stroke, heart failure/post-MI, ALS, and neonatal brain injury, as well as the importance of Muse cell enrichment (≥70–75% purity) for maximal benefit, since mixed MSC populations often dilute or inhibit Muse-specific benefits.
Clinical cases illustrated the real-world application:
- A lumbar disc collapse with marrow edema was treated using epidural exosomes, resulting in resolution of bone edema and significant pain relief.
- A shoulder supraspinatus tear treated with Muse cells and exosomes, which incidentally appeared to benefit the patient’s lumbar spine issues—likely due to systemic homing of these regenerative signals.
Finally, we discussed recovery and optimization, including the importance of avoiding NSAIDs, strategically using peptides and mitochondrial supports, and emphasizing sleep, nutrition, and rehabilitative movement. Regenerative therapies act as catalysts, but long-term success depends on the patient’s day-to-day environment and systemic balance.
Conclusion
The future of spine and neuroinflammation care lies in integrated, systems-based, and regenerative approaches. Structural problems—disc degeneration, facet arthropathy, nerve irritation—must be addressed, but they cannot be viewed in isolation from systemic inflammation, immune status, mitochondrial health, and postural mechanics. Modern research on cellular senescence, Muse cells, exosomes, and peptides gives us powerful tools to modulate these deeper layers.
My approach is to sequence care: evaluate comprehensively, prepare the biological terrain, apply precise regenerative therapies, and then support recovery with targeted nutrition, peptides, and rehabilitation. Throughout, I emphasize quality and safety in diagnostic methods, in therapeutic products, and in procedure execution.
As the evidence base expands, I expect therapies like Muse cells to play a major role in conditions once considered largely irreversible: chronic spinal degeneration, post-stroke disability, heart failure, and selected neurodegenerative disorders. Yet even as these advanced therapies mature, the fundamentals—proper diagnosis, lifestyle, biomechanics, and individualized care—remain essential.
For patients, the key message is that chronic spine and neuroinflammatory symptoms are rarely “just in your neck” or “just in your back.” A comprehensive, evidence-based plan can address both the local structures and the systemic drivers that determine whether you truly heal or remain trapped in a cycle of pain.
Key Insights
- Spine pain is systemic. Disc and facet pathology often coexist with neuroinflammation, gut dysfunction, toxin burden, and autonomic imbalance.
- Posture and ligament laxity matter. Forward head posture and connective tissue disorders can drive cervical instability, vagus nerve dysfunction, TMJ pain, and vestibular symptoms.
- Inflammation has subtypes. Distinguishing non-sterile (infection-driven) from sterile (damage- and senescence-driven) inflammation is crucial for effective treatment.
- Senescence is not always bad. Early P21-type senescence contributes to normal healing, whereas chronic P16-dominant “zombie cells” drive persistent sterile inflammation and degeneration.
- Prepare before you regenerate. Optimizing mitochondria, nutrients, hormones, immune balance, and detox pathways increases the success of regenerative therapies.
- Quality is non-negotiable. Peptides and biologics must be sourced from reliable, tested, cGMP-compliant suppliers to avoid adverse reactions and therapeutic failure.
- Muse cells are a promising frontier. They are pluripotent-like, stress-enduring, non-tumorigenic, and capable of homing to injury sites, differentiating into local cell types, and functioning allogeneically via HLA-G.
- Enrichment matters. Muse cells must be sufficiently purified to avoid being overshadowed by non-Muse MSC populations.
- Clinical cases support potential. Early experiences with Muse cells and exosomes in spinal and shoulder conditions show promising structural and symptomatic improvements.
- Recovery is an active process. Avoiding NSAIDs, using targeted peptides and mitochondrial supports, and focusing on sleep, nutrition, and posture are all essential to long-term success.
Keywords
Spine pain, facet arthropathy, disc degeneration, neuroinflammation, functional medicine, glymphatic system, forward head posture, cervical instability, vagus nerve dysfunction, TMJ pain, tinnitus, vertigo, autonomic dysfunction, sterile inflammation, non-sterile inflammation, PAMPs, DAMPs, cellular senescence, P21 senescence, P16 senescence, zombie cells, mitochondrial dysfunction, peptides, solid-phase peptide synthesis, vector-based peptide production, Muse cells, multilineage-differentiating stress-enduring cells, HLA-G, exosomes, regenerative medicine, myocardial infarction, stroke, ALS, bone marrow edema, MRI, gut dysbiosis, toxin burden, mold, heavy metals, mitochondrial support, BPC-157, TB-500, GHK-Cu, SS-31, regenerative spine care, evidence-based integrative medicine.
Disclaimer
This educational content is provided by Dr. Alex Jimenez, DC, FNP-APRN, for informational and educational purposes only. It is not intended as medical advice, diagnosis, or treatment, nor does it substitute for individualized medical care.
All individuals must seek and follow personalized recommendations from their own licensed healthcare providers, who can take into account their unique medical history, current medications, diagnostic findings, and overall health status. Do not start, stop, or change any treatment based on this information without consulting your personal medical provider.
Post Disclaimer
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Regenerative Therapies and Solutions for Neuroinflammation" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine; wellness; contributing etiological viscerosomatic disturbances within clinical presentations; associated somato-visceral reflex clinical dynamics; subluxation complexes; sensitive health issues; and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and licensure jurisdiction. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that directly or indirectly relate to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
New Mexico CNP License#: 90560, Verified
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
| Yes | 363LF0000X - Nurse Practitioner - Family | NM |
90560 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
📆 Schedule Appointment: Schedule 24/7 (Click Here)