


Anxiety is the most common mental health disorder in the United States, impacting more than 40 million adults. Though some instances can be moderate and short-lived, others may be painfully debilitating, lasting for years, or becoming a chronic problem. While almost anyone can experience temporary anxiety before a variety of events, anxiety is regarded as problematic when it starts to interfere in one way or another with regular, everyday function, including sleep disturbances, social stress, or self-care. Anxiety is connected to a number of lifestyle, health, and nutritional aspects, but understanding the triggers and root causes can result in a more effective treatment approach.
The thought of the existence of an interaction between the immune system and the central nervous system, or CNS, has prompted extensive research attention into the subject of “psychoneuroimmunology”, carrying the area to an intriguing level where new hypotheses are being increasingly tested. So far, the presence of inflammatory reactions and the crucial effects of depression have received most attention. But considering a large socioeconomic impact due to an alarming increase in anxiety disorder patients, there is an urgent research need for better comprehension of the role of inflammation in anxiety and how this relationship can influence one another. The purpose of the article below is to demonstrate the results as well as discuss the outcome measures of a large cohort study conducted in order to determine the possible connection between anxiety disorders and brain inflammation.
Table of Contents
Anxiety Disorders and Inflammation in a Large Adult Cohort
Abstract
Although anxiety disorders, like depression, are increasingly being associated with metabolic and cardiovascular burden, in contrast with depression, the role of inflammation in anxiety has sparsely been examined. This large cohort study examines the association between anxiety disorders and anxiety characteristics with several inflammatory markers. For this purpose, persons (18–65 years) with a current (N=1273) or remitted (N=459) anxiety disorder (generalized anxiety disorder, social phobia, panic disorder, agoraphobia) according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition criteria and healthy controls (N=556) were selected from the Netherlands Study of Depression and Anxiety. In addition, severity, duration, age of onset, anxiety subtype and co-morbid depression were assessed. Inflammatory markers included C-reactive protein (CRP), interleukin (IL)-6 and tumor-necrosis factor (TNF)-?. Results show that after adjustment for sociodemographics, lifestyle and disease, elevated levels of CRP were found in men, but not in women, with a current anxiety disorder compared with controls (1.18 (s.e.=1.05) versus 0.98 (s.e.=1.07) mg?l?1, P=0.04, Cohen’s d=0.18). No associations were found with IL-6 or TNF-?. Among persons with a current anxiety disorder, those with social phobia, in particular women, had lower levels of CRP and IL-6, whereas highest CRP levels were found in those with an older age of anxiety disorder onset. Especially in persons with an age of onset after 50 years, CRP levels were increased compared with controls (1.95 (s.e.=1.18) versus 1.27 (s.e.=1.05) mg?l?1, P=0.01, Cohen’s d=0.37). In conclusion, elevated inflammation is present in men with current anxiety disorders. Immune dysregulation is especially found in persons with a late-onset anxiety disorder, suggesting the existence of a specific late-onset anxiety subtype with a distinct etiology, which could possibly benefit from alternative treatments.
Keywords: anxiety disorder, anxiety characteristics, cohort study, inflammation
Introduction
Anxiety disorders are among the most prevalent and disabling mental disorders.1, 2 Increasing evidence links anxiety to cardiovascular risk factors and diseases such as atherosclerosis,3 metabolic syndrome,4 and coronary heart disease.5, 6 As low-grade systemic inflammation is clearly involved in the etiology of these somatic conditions,7, 8, 9 it has been hypothesized that inflammation has a role in anxiety disorders and may form the link between anxiety disorders and cardiovascular burden.10 Anxiety disorders are also highly co-morbid with depression,11 which has recurrently been associated with immune dysregulation.12, 13 However, unlike depression, very few studies have investigated the relationship between anxiety disorders and inflammation. Two recent studies have correlated anxiety symptoms with increased cytokine levels, in particular C-reactive protein (CRP).14, 15 With regard to anxiety disorders, research has mainly focused on posttraumatic stress disorder, in which high levels of inflammatory markers have been found.16, 17 Sparse evidence from relatively small clinical studies (n?100) suggests increased inflammatory activation in patients with panic disorder18 and generalized anxiety disorder,19 which seems to be independent of co-morbid depression.
As there is yet limited research on immune dysregulation and anxiety, one can only speculate on the mechanisms linking these two conditions. Experimentally induced stress has been shown to produce an inflammatory reaction,20 which has led researchers to suggest that it is in particular the experience of acute stress, such as present in panic disorders, causing the high levels of inflammation in anxiety.18 On the other hand, chronic stress may initiate changes in the hypothalamic–pituitary–adrenal (HPA) axis and the immune system, which in turn can trigger depression as well as anxiety.21 These pathways are not independent as the HPA-axis and the immune system are closely linked. Although the HPA axis in normal situations should temper inflammatory reactions, prolonged hyperactivity of the HPA axis could result in blunted anti-inflammatory responses to glucocorticoids resulting in increased inflammation.22, 23 Likewise, it can be hypothesized that immune changes associated with chronic disease and aging,24 could induce similar anxiety-enhancing effects. Although several mechanisms might explain an association between inflammation and anxiety disorders, it can be expected that immune dysregulation is not a general phenomenon in anxiety disorders, but might be restricted to specific subgroups. Whether this anxiety subgroup is defined by the type of disorder, the severity or duration of the disorder, the co-morbidity with depression, or its age of onset, is yet to be examined.
The present study investigates the association between several common anxiety disorders (generalized anxiety disorder, social phobia, panic disorder, agoraphobia) and heightened inflammation (CRP, interleukin (IL)-6, tumor necrosis factor (TNF)-?) in a large sample of persons with current and remitted anxiety disorders and healthy controls. In addition, it will be examined whether specific anxiety characteristics (severity, duration, age of onset, subtype, depression co-morbidity) further discriminate those anxiety patients with elevated inflammation.
Subjects and Methods
Sample
The Netherlands Study of Depression and Anxiety (NESDA) includes 2981 persons with and without depressive and anxiety disorders, aged 18–65 years at the baseline assessment in 2004–2007. Participants were recruited from the community (19%), general practice (54%) and secondary mental health care (27%) in order to reflect the broad range and developmental trajectory of psychopathology. Persons with insufficient command of the Dutch language or a primary clinical diagnosis of bipolar disorder, obsessive compulsive disorder, severe substance use disorder, psychotic disorder or organic psychiatric disorder, as reported by themselves or their mental health practitioner, were excluded. A detailed description of the NESDA study design and sampling procedures can be found elsewhere.25 The research protocol was approved by the ethics committee of participating universities and after complete description of the study all respondents provided written informed consent.
During the baseline interview, the presence of anxiety disorder (generalized anxiety disorder, social phobia, panic disorder, agoraphobia) and depressive disorder (major depressive disorder, dysthymia) was established using the Composite Interview Diagnostic Instrument (CIDI) according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition criteria.26 The CIDI is a highly reliable and valid instrument for assessing depressive and anxiety disorders27 and was administered by specially trained research staff. In addition, the severity of anxiety was measured in all participants using the 21-item self-report Beck Anxiety Inventory.28 For the present analyses, we selected persons with a current (that is, past 6 months) or remitted (lifetime, but not current) anxiety disorder and healthy controls. Healthy controls had no lifetime anxiety or depressive disorder and a Beck Anxiety Inventory score below 10, as a score of 10 or above indicates mild anxiety.29 Persons with anxiety disorders were allowed to have a co-morbid depression. Of these 2342 persons, 54 were excluded due to missing information on inflammatory markers, leaving a sample of 2288 persons for the present study. Persons with missing data on inflammation were less often female (55.6 versus 66.9%, P=0.08), but did not differ from included persons in terms of age, years of education and the presence of anxiety disorder.
Anxiety Characteristics
Next to subtype of CIDI anxiety disorder diagnosis (generalized anxiety disorder, social phobia, panic disorder, agoraphobia), anxiety characteristics included anxiety symptoms severity as measured by the Beck Anxiety Inventory, and anxiety symptoms duration, using the Life Chart Interview (LCI).30 The LCI uses a calendar method to determine life events during the past 4 years to refresh memory after which the presence of anxiety and avoidance symptoms during that period is assessed. From this, the per cent of time patients reported anxiety symptoms was computed. The LCI has been used by other large cohort studies31 and event history calendars such as the LCI have been suggested a natural method of choice for retrospective data collection.32 To be able to test whether inflammation was in particular associated with anxiety disorders with a later onset, as we had found for depression,33 age of anxiety onset was derived from the CIDI interview. Last, the presence of a current co-morbid depressive disorder (major depressive disorder, dysthymia) was taken from the CIDI to check whether a possible inflammation–anxiety association was independent of co-morbid depression.
Inflammatory Markers
Markers of inflammation were assessed at the baseline NESDA measurement and included CRP, IL-6 and TNF-?. Fasting blood samples of NESDA participants were obtained in the morning between 0800 and 0900 hours and kept frozen at ?80?°C. CRP and IL-6 were assayed at the Clinical Chemistry Department of the VU University Medical Center. High-sensitivity plasma levels of CRP were measured in duplicate by an in-house ELISA based on purified protein and polyclonal anti-CRP antibodies (Dako, Glostrup, Denmark). Intra- and inter-assay coefficients of variation were 5% and 10%, respectively. Plasma IL-6 levels were measured in duplicate by a high sensitivity ELISA (PeliKine CompactTM ELISA, Sanquin, Amsterdam, The Netherlands). Intra- and inter-assay coefficients of variation were 8% and 12%, respectively. Plasma TNF-? levels were assayed in duplicate at Good Biomarker Science, Leiden, The Netherlands, using a high-sensitivity solid phase ELISA (Quantikine® HS Human TNF-? Immunoassay, R&D systems, Minneapolis, MN, USA). Intra- and inter-assay coefficients of variation were 10% and 15%, respectively.
Covariates
Sociodemographic characteristics included sex, age and years of education. As lifestyle characteristics can be associated with both anxiety and inflammation, smoking status (never, former, current), alcohol intake (<1, 1–14 (women)/1–21 (men), >14 (women)/>21 (men) drinks per week), physical activity (measured with the International Physical Activity Questionnaire34 in MET-minutes (ratio of energy expenditure during activity compared with rest times the number of minutes performing the activity) per week) and body mass index (weight in kilograms divided by height in meters squared) were assessed. In addition, several disease-related covariates were taken into account including the presence of cardiovascular disease (assessed by self-report supported by appropriate medication use (see Vogelzangs et al.6 for detailed description)), the presence of diabetes (fasting plasma glucose level ?7.0?mmol?l?1 or use of anti-diabetic medication (ATC code A10)) and the number of other self-reported chronic diseases for which persons received treatment (including lung disease, osteoarthritis or rheumatic disease, cancer, ulcer, intestinal problem, liver disease, epilepsy and thyroid gland disease). Medication use was assessed based on drug container inspection of all drugs used in the past month and classified according to the World Health Organization Anatomical Therapeutic Chemical classification.35 Statin use (C10AA, C10B) and use of systemic anti-inflammatory medication (M01A, M01B, A07EB, A07EC) were assessed. Antidepressant medication included regular use (>50% of the time) of selective serotonin reuptake inhibitors (SSRI; N06AB), serotonin-norepinephrine reuptake inhibitors (SNRI; N06AX16, N06AX21), tricyclic antidepressants (TCA; N06AA) and tetracyclic antidepressants (TeCA; N06AX03, N06AX05, N06AX11).
Statistical Analyses
Baseline characteristics were compared between men and women using ?2 test for dichotomous and categorical variables, independent samples t-test for continuous variables, and Mann–Whitney U-test for inflammatory markers. For subsequent analyses, CRP, IL-6 and TNF-? were ln-transformed to normalize distributions, but back-transformed values are presented to enhance interpretation. Associations between anxiety disorders and inflammatory markers were examined using analyses of (co)variance, and (adjusted) means across anxiety groups (no, remitted, current) are presented. To take the effects of potential confounding factors into account, three different models were tested: unadjusted, adjusted for sociodemographics (sex, age, education) and additionally adjusted for lifestyle and disease (smoking status, alcohol intake, physical activity, body mass index, cardiovascular disease, diabetes, number of other chronic diseases, statins, anti-inflammatory medication). As depression has been reported to differentially affect inflammation in men and women,33 a sex-interaction for anxiety disorders is plausible. Therefore, we tested sex-interactions by including a sex × anxiety disorder status interaction term. When present, analyses were repeated sex stratified.
To test whether specific anxiety characteristics were related to elevated inflammation levels, we performed linear regression analyses with inflammatory markers as the outcome for each anxiety characteristic (severity, duration, age of onset, subtype, depression co-morbidity) within the sample of persons with a current anxiety disorder.
Dr. Alex Jimenez’s Insight
Anxiety is a common term which is often used to refer to situational stress or to describe momentary tenseness, however, for individuals living with an anxiety disorder, the symptoms associated with this mental health issue can be debilitating. Anxiety can be caused by a wide variety of factors, including depression and chronic pain, however, research studies have started to hypothesize that another common factor may be the true source as to why some people develop anxiety while other don’t: inflammation. The connection between anxiety and inflammation, as well as depression and inflammation, is becoming increasingly understood. Anxiety isn’t likely caused by inflammation alone, but, measuring inflammatory levels in the body could help determine the best treatment approach for a variety of anxiety disorders and for underlying health issues most commonly associated with inflammation, such as chronic pain.
Results
Mean age of the study sample was 41.8 (s.d.=13.1) years and 66.9% were women. Baseline characteristics of the total sample and for men and women separately are shown in Table 1. Women were younger, more often non-drinkers, had a lower body mass index, less often cardiovascular disease or diabetes and less often used statins than men. In addition, women had higher levels of CRP than men. All covariates were associated with at least one of the inflammation markers, which has been presented elsewhere.33 Pearson’s correlations between inflammatory markers were modest (CRP–IL-6: r=0.31; CRP–TNF-?: r=0.13; IL-6–TNF-?: r=0.12; all P<0.001).
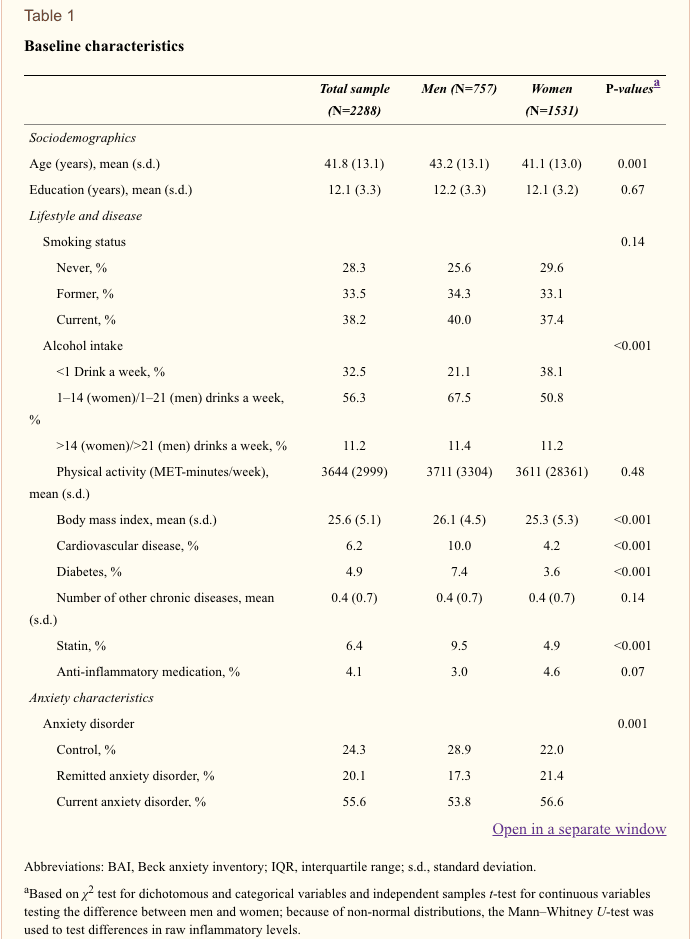
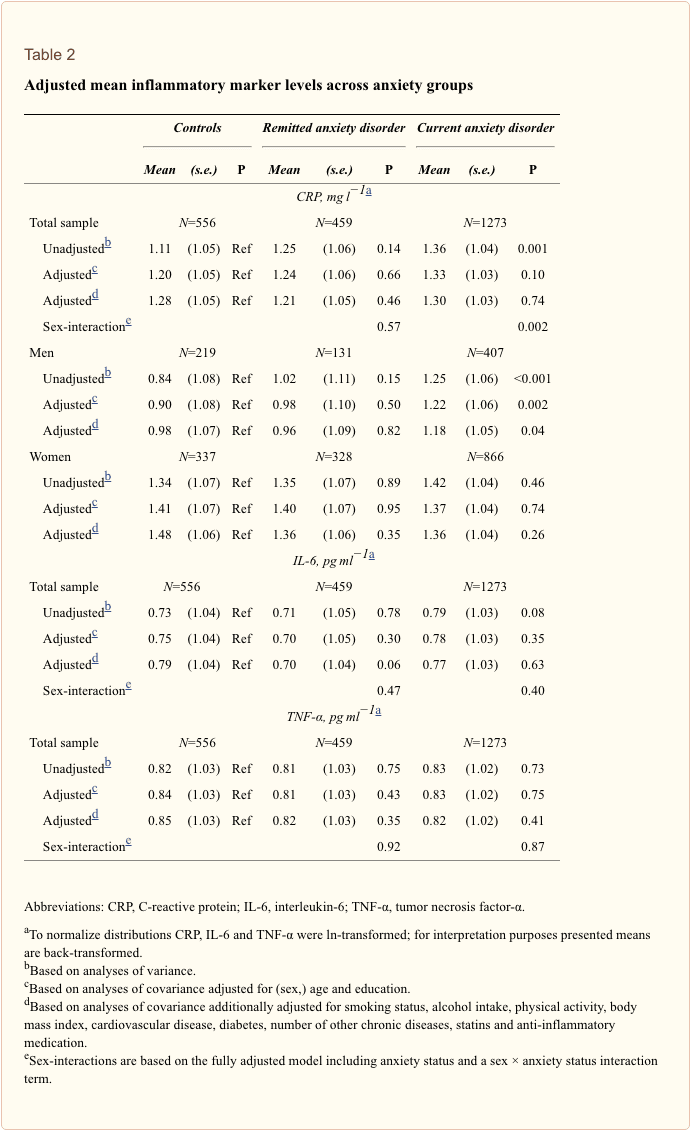
Table 2 shows (adjusted) mean inflammation levels across anxiety groups (controls, remitted, current) based on analyses of (co)variance. In the total sample, higher CRP levels were found in persons with a current anxiety disorder compared with controls in unadjusted analyses (1.36 (s.e.=1.04) versus 1.11 (s.e.=1.05) mg?l?1, P=0.001), but after adjustment, there were no associations between anxiety disorders and any of the inflammation markers. However, a significant sex × anxiety disorder interaction was found for CRP (remitted: P=0.57; current: P=0.002). Stratified analyses for CRP showed that even after full adjustment for lifestyle and disease, men with current anxiety disorders had higher levels of CRP compared with controls (1.18 (s.e.=1.05) versus 0.98 (s.e.=1.07) mg?l?1, P=0.04, Cohen’s d=0.18). In women, anxiety disorders were not significantly associated with CRP. No sex interactions were found for IL-6 (remitted: P=0.47; current: P=0.40) or TNF-? (remitted: P=0.92; current: P=0.87). As we have previously reported associations between inflammatory levels and antidepressant use within currently depressed persons,33 we checked the influence of antidepressant use on our current results. Higher levels of CRP were found in TCA/TeCA users within our present sample of persons with current anxiety disorders (N=1273; P=0.001). To examine whether the finding of elevated CRP in currently anxious men was independent of TCA/TeCA use, we excluded all men using TCA/TeCA (N=36). Results remained similar, although no longer significant (men with current anxiety disorders versus controls: 1.13 (s.e.=1.05) versus 0.97 (s.e.=1.07) mg?l?1, P=0.08, Cohen’s d=0.15). In addition, to reduce the possible confounding effects of acute illness on inflammatory levels at the time of blood draw, all persons who reported having had a cold or fever in the week before blood draw were excluded (N=645), but findings remained alike (men with current anxiety disorders versus controls: 1.09 (s.e.=1.06) versus 0.91 (s.e.=1.07) mg?l?1, P=0.06, Cohen’s d=0.19).
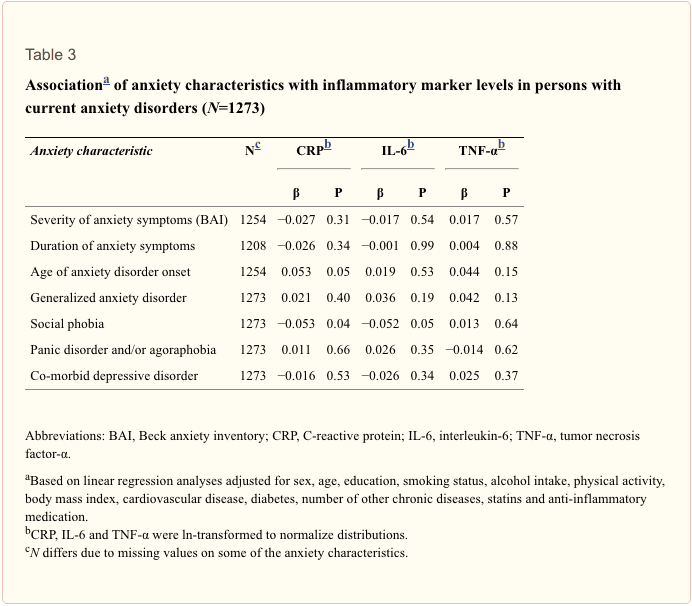
To investigate whether specific anxiety characteristics (severity, duration, age of onset, subtype, depression co-morbidity) were associated with inflammation, linear regression analyses were performed within the subgroup of persons with current anxiety disorders (N=1273; Table 3). Anxiety severity and duration did not correlate with inflammation. Later age of anxiety disorder onset was associated with elevated CRP levels (?=0.053, P=0.05), even after additional adjustment for TCA/TeCA use (?=0.053, P=0.05). Persons with social phobia had lower levels of CRP (?=?0.053, P=0.04) and IL-6 (?=?0.052, P=0.05) compared with persons with other types of anxiety disorders. The association between social phobia and IL-6 appeared to be specific for women (?=?0.089, P=0.007), but not men (?=0.025, P=0.61; P sex-interaction=0.05). Co-morbid depressive disorder did not further differentiate anxious persons with elevated inflammation.
To further illustrate the findings with regard to age of onset, we constructed five age of anxiety disorder onset groups (<20, 20–30, 30–40, 40–50, ?50). Figure 1 presents adjusted means of back-transformed CRP levels across controls and age of onset groups based on analysis of covariance. CRP levels were only increased in persons with an age of onset after 50 years (1.95 (s.e.=1.18) versus 1.27 (s.e.=1.05) mg?l?1 in controls, P=0.01, Cohen’s d=0.37). For comparison, adjusted mean CRP levels for persons with cardiovascular disease were 1.62 (s.e=1.11), illustrating the clinical relevance of this finding. Excluding persons reporting having had a cold or fever in the week before blood draw (N=513), yielded similar findings (age of onset after 50 years versus controls: 1.73 (s.e.=1.20) versus 1.18 (s.e.=1.05) mg?l?1, P=0.04, Cohen’s d=0.35). Results were also similar when the analysis of Figure 1 was restricted to the sample of persons aged 50 years or above (N=589; age of onset after 50 years versus controls: 2.05 (s.e.=1.16) versus 1.35 (s.e.=1.08) mg?l?1, P=0.01, Cohen’s d=0.40), underlining that higher CRP in those with an age of onset of 50 years or above was not due to the higher age itself in these persons. Last, in a post-hoc analysis, we directly compared CRP levels between persons with a late versus early onset of anxiety disorder at a cutoff of 50 years, and found significantly higher CRP levels in the late onset group (1.91 (s.e.=1.19) versus 1.35 (s.e.=1.03) mg?l?1, P=0.05, Cohen’s d=0.30).

Discussion
The current study is one of the first and the largest to date to examine the association between anxiety disorders and inflammation. The results show that men with a current anxiety disorder have somewhat increased levels of CRP, even after taking a large set of lifestyle and disease factors into account. Elevated levels of CRP were in particular found in those persons with a late onset of the anxiety disorder.
Our results are in line with the few previous studies examining the relationship between anxiety symptoms or disorders with inflammation. Available evidence until now was limited to assessing anxiety symptoms in the general population,14, 15 confined to specific anxiety disorders in small clinical samples16, 17, 18 or in a heart disease population.19 Our study adds to the literature by showing that elevated CRP levels can be found among several common anxiety disorders in a relatively large cohort of anxious persons and controls, specifically in those with a later onset of the anxiety disorder. CRP levels were in particular elevated among men with anxiety disorders, which is in line with the large-scale study by Liukkonen et al.,15 which showed an association between anxiety symptoms and CRP only in men. In contrast, Pitsavos et al.14 found associations between an anxiety symptoms score and CRP levels in both men and women. Persons included in the study by Pitsavos et al. were much older (18–89 years; mean age 45 years) than those in the study by Liukkonen et al. (all 31 years old), and slightly older than those in the present study (18–65 years; mean age 42 years). Perhaps sex differences become less clear with increasing age, as a result of hormonal changes across the lifespan of women, which affect inflammation levels.36 This could be in line with our finding that CRP levels were elevated in both men and women with a late onset of anxiety disorders.
Our findings with respect to anxiety disorders are also very comparable to our earlier findings regarding depressive disorders and inflammation.33 In that study, we found elevated inflammation, specifically CRP, in depressed men, especially among those with a later depression onset. The effect sizes for CRP in men with a current disorder are also comparable for anxiety (Cohen’s d=0.18) and depressive (Cohen’s d=0.21) disorders. A trend for association with IL-6, which was found for current depressive disorders in men, was not found for current anxiety disorders. Of note is that in persons with an anxiety disorder, a co-morbid depressive disorder was not associated with higher inflammation levels, suggesting that the effects found for anxiety disorders are independent of depression.
In line with our previous findings for current depressive disorders,33 CRP levels were in particular elevated among persons with a later onset of anxiety disorders. In contrast, characteristics that are more often associated with an early age of onset, such as higher severity and longer duration were not associated with increased inflammation. Also, in our sample, women had an earlier age of anxiety disorder onset than men, possibly contributing to the lack of an overall association between anxiety disorders and inflammation in women. Furthermore, we found that CRP levels were lowest among persons with social phobia when compared with other anxiety disorders, in particular in women. Social phobia has been reported to have a much earlier age of onset compared with generalized anxiety disorder or panic disorder,37 which was confirmed in our sample (16.6 versus 25.9 years, P<0.001). To our knowledge, no other study has yet examined the association between social phobia and inflammation. In our study, only nine persons with social phobia had an disorder onset at or after 50 years. Therefore, low inflammation levels in persons with social phobia cannot explain our findings for elevated CRP levels in persons with an age of anxiety disorder onset after 50 years. A recent study by Copeland et al.38 showed that, after taking health-related behaviors into account, generalized anxiety disorder was not associated with elevated CRP levels among children and adolescents. These findings argue against the idea that the inflammation–anxiety association is merely a result of acute stress experienced in anxiety disorders. Although we cannot make inferences about etiology based on our cross-sectional analyses, our current findings are in line with the growing evidence suggesting a distinct etiology involving vascular/metabolic/inflammatory factors in depression or anxiety disorders with an onset later in life.39, 40, 41, 42 Possibly, accumulating psychological and physical stress across the life-span might induce immunological changes24 that eventually results in depression and anxiety.
In our previous report,33 we had found differences in inflammation levels among different classes of antidepressant medication use, which was confirmed for higher CRP in TCA/TeCA users within our present sample of persons with current anxiety disorders. Excluding persons using TCA or TeCA, resulted in a slightly weaker effect size for the association between current anxiety disorder and CRP in men. This might suggest that the elevated CRP levels in men with current anxiety disorders are for some part due to use of TCA/TeCA. On the other hand, persons using TCA/TeCA might represent the more severe cases of anxiety disorders, in which case exclusion of these persons leads to an underestimation of the association. Adjustment for TCA/TeCA use had no effect on our findings for age of anxiety disorder onset, suggesting that late-onset anxiety disorders are independently associated with higher levels of CRP.
What are the clinical implications of our findings? First, our finding of increased CRP levels in particularly those with a late onset of the anxiety disorder might implicate the existence of a specific late-onset anxiety subtype with a distinct etiology. As we have found similar results for depression33 and because depression and anxiety are highly co-morbid disorders,11 this might suggest that depression and anxiety with a late onset share a similar etiology and represent one particular group of disorders, which might be more distinct from other depressive or anxiety disorders, which present earlier in life. As we can only speculate on etiology based on our cross-sectional research, longitudinal research is needed to validate the existence of an etiologically distinct late-onset subtype. Second, if confirmed, a distinct etiology for late-onset disorders implicates different treatment strategies for this subgroup. Perhaps anti-inflammatory medication or lifestyle interventions, such as exercise, for which (some) evidence exists that they normalize immune and metabolic dysregulation,43 as well as improve depressive symptoms to some degree,44, 45 could be beneficial in persons with late onset anxiety disorders as well.
Our study has some important strengths such as a large sample size, assessment of multiple inflammatory markers, clinical diagnoses of several anxiety disorders, adequate adjustment for potential confounders and the ability to examine the role of anxiety characteristics. However, some limitations need to be acknowledged. As our data are cross-sectional, we cannot make any inferences about the direction of the association. Also, although we adjusted for a large set of possible confounding factors, unmeasured poor lifestyle behaviors or health factors may be the explaining link between inflammation and anxiety disorders. For instance, subclinical cardiovascular disease could possibly precede both inflammation and anxiety. On the other hand, subclinical disease may be one pathway of how inflammation leads to anxiety in later life. Longitudinal studies are needed to investigate whether immune dysregulation is a precursor or the result of anxiety, or whether this relationship is bidirectional. Further, like most other studies, we assessed circulating levels of inflammatory markers, which show a high degree of intra-individual variation that could explain the rather modest overall associations between anxiety disorders and inflammation in our study.
In conclusion, our results show that low-grade systemic inflammation is present in men with anxiety disorders. Elevated inflammation is in particular found in both men and women with the onset of anxiety disorder later in life. Longitudinal studies are needed to confirm inflammation as an etiological factor in anxiety disorders with a late-life onset, followed by intervention trials investigating new treatment strategies (for example, anti-inflammatory medication, lifestyle interventions) for this subset of persons with late-onset anxiety.
Acknowledgments
The infrastructure for the NESDA study (http://www.nesda.nl) is funded through the Geestkracht program of the Netherlands Organisation for Health Research and Development (Zon-Mw, grant number 10-000-1002) and is supported by participating universities and mental health care organizations (VU University Medical Center, GGZ inGeest, Arkin, Leiden University Medical Center, GGZ Rivierduinen, University Medical Center Groningen, Lentis, GGZ Friesland, GGZ Drenthe, Institute for Quality of Health Care (IQ Healthcare), the Netherlands Institute for Health Services Research (NIVEL) and the Netherlands Institute of Mental Health and Addiction (Trimbos)). NV was supported through a fellowship from the EMGO Institute for Health and Care Research and BP through a VICI grant (NWO grant g1811602). Assaying of inflammatory markers was supported by the Neuroscience Campus Amsterdam.
Notes
The authors declare no conflict of interest.
Beyond CBD – Supporting the Entire Endocannabinoid System
Every day, more and more health-conscious consumers are starting to take great interest in nutritional supplements that encourage the proper function of the endocannabinoid system, or ECS. Although marijuana and substances derived from or related to marijuana were believed to be the only options to achieve this effect, the focus in the consumer market has largely shifted to a single chemical: cannabidiol.
What’s CBD?
Cannabidiol, commonly known as CBD, is a chemical found in marijuana and in hemp which does interact with the ECS. CBD is just one of a wide group of chemicals known as phytocannabinoids. Cannabidiol has turned into a well-known phytocannabinoid because it is being researched to turn into a new medication and also the benefits demonstrated by CBD have created a lot of attention in this compound.
What Can CBD Do?
Although CBD does perform multiple actions within the human body, its own best-known function in the ECS, or endocannabinoid system, is in its potential to inhibit the activity of the enzyme called fatty acid amide hydrolase, or FAAH. FAAH breaks down anandamide, among the body’s endogenous cannabinoids, which is known to bind to the ECS’s CB1 receptor. The ECS’s CB1 receptor, primarily found in the brain, is the exact same receptor which THC, or tetrahydrocannabinol, binds to. In other words, anandamide, often referred to as “the bliss molecule”, is the human body’s natural THC.
Significantly, however, whereas THC could have negative effects, such as triggering feelings of anxiety, mild hallucinations, dizziness, rapid heart rate, slowed reaction times, and food cravings, the anandamide made naturally by the body appears to exert positive effects on mood, memory, brain function and pain. Because anandamide is normally rapidly broken up by FAAH and because CBD modulates FAAH, Cannabidiol’s primary importance is in the way it can maintain anandamide levels, thus enhancing anandamide’s beneficial impact in the ECS. CBD also binds directly to CB1 and CB2 receptors and has a selection of activity outside of the ECS which can result in its many health benefits.
CBD is a Drug According to the FDA
Because CBD is comparatively safe, lacks the unwanted side effects of THC, and may be easily derived from hemp instead of marijuana, the natural products industry was flooded with products labeled as CBD. However, before this recent phenomenon, a British pharmaceutical company began studying the merits of CBD as an alternate to the drugs and/or medications being utilized to treat resistant childhood epilepsy.
This company, GW Pharmaceuticals (dba Greenwich Biosciences) began pre-clinical operations on CBD in 2007 and contains an investigational new drug called Epidiolex® in late stage clinical trials.
In multiple warning letters in 2017 sent to a number of businesses, the FDA noted ,”If an article, such as CBD, has been approved for investigation as a new drug and/or medication for which substantial clinical investigations have been instituted and for which the existence of such investigations have been made public, then products containing that chemical are outside the definition of a dietary supplement” Since the investigational work completed on CBD as a drug predates the promotion of CBD as a dietary supplement, products containing purified CBD or enriched with CBD are considered by the FDA to be medication and not dietary supplements.
Why Support the Entire ECS?
The ECS is not just a bodily system which completes a single function, as a matter of fact it’s far from it. ECS receptors are widely dispersed throughout the entire body. CBD is an isolated molecule which acts primarily on just a single component of the ECS; i.e., it inhibits the degrading enzyme FAAH, thus allowing the anandamide naturally produced by your endocannabinoid system to possess higher action. But what about the rest of the ECS?
The ECS has at least two major receptors, CB1 and CB2 receptors. And along with anandamide, humans also produce an endocannabinoid called 2-archidonoyl glycerol, or 2-AG, which can be degraded by the enzyme monoacylglycerol lipase, or MAGL. If our intention is to support and nourish the whole ECS, then focusing on a single molecule like CBD that only works on one portion of the ECS might not be the best approach.
Hemp includes heaps of active molecules, including a range of phytocannabinoids. Some such as cannabigerol, or CBG, bind weakly to the CB1 and CB2 receptors. Both CBG and cannabichromene, or CBC, may also help maintain wholesome anandamide levels. The phytocannabinoid beta-caryophyllene, or BCP, that is found in plants like black pepper and clove, binds to the CB2 receptor, which supports the actions of 2AG. Other natural plant compounds, particularly specific terpenoids, have functions which are complementary to that of phytocannabinoids.
The “Entourage” Impact
Although isolated CBD does have a part in overall health and wellness, cannabidiol is not anywhere near the entire process for encouraging the ECS. By using a whole hemp stalk infusion combined with hops, pepper, clove and rosemary that include naturally occurring complementary compounds, hemp oil nourishes the whole ECS, giving a holistic approach to a system that’s often neglected and out of equilibrium in today’s stressful world.
Hemp oil nourishes the entire ECS, giving a holistic approach to a system that’s frequently ignored and out of equilibrium in today’s stressful world. Scientists who research the ECS refer to the approach as the”entourage” effect, and several top researchers believe this approach to be extremely effective in keeping the health and tone of the valuable endocannabinoid system as well as controlling the symptoms of inflammation and anxiety in the human body.
In conclusion, anxiety is one of the most common mental health disorders in the United States. This debilitating health issue can be caused by a variety of factors, however, many research studies have started to demonstrate a connection between anxiety disorders and brain inflammation. According to the article above, stress has been shown to produce an inflammatory reaction, which has led researchers to suggest that anxiety may be causing high levels of inflammation. The outcome measures of te cohort study found that low-grade inflammation is present in individuals with anxiety disorders. Further research studies are still required to confirm the connection between anxiety and inflammation. Furthermore, supporting the function of the endocannabinoid system, or ECS, with the use of CBD or cannabidiol, has been found to have many health benefits, including helping with inflammation and anxiety. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
1. Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:617–627. [PMC free article] [PubMed]
2. Buist-Bouwman MA, de GR, Vollebergh WA, Alonso J, Bruffaerts R, Ormel J. Functional disability of mental disorders and comparison with physical disorders: a study among the general population of six European countries. Acta Psychiatr Scand. 2006;113:492–500. [PubMed]
3. Seldenrijk A, Vogelzangs N, van Hout HP, van Marwijk HW, Diamant M, Penninx BW. Depressive and anxiety disorders and risk of subclinical atherosclerosis Findings from the Netherlands Study of Depression and Anxiety (NESDA) J Psychosom Res. 2010;69:203–210. [PubMed]
4. Carroll D, Phillips AC, Thomas GN, Gale CR, Deary I, Batty GD. Generalized anxiety disorder is associated with metabolic syndrome in the Vietnam experience study. Biol Psychiatry. 2009;66:91–93. [PubMed]
5. Roest AM, Martens EJ, de JP, Denollet J. Anxiety and risk of incident coronary heart disease: a meta-analysis. J Am Coll Cardiol. 2010;56:38–46. [PubMed]
6. Vogelzangs N, Seldenrijk A, Beekman AT, van Hout HP, de JP, Penninx BW. Cardiovascular disease in persons with depressive and anxiety disorders. J Affect Disord. 2010;125:241–248. [PMC free article] [PubMed]
7. Libby P. Inflammation in atherosclerosis. Nature. 2002;420:868–874. [PubMed]
8. Sutherland JP, McKinley B, Eckel RH. The metabolic syndrome and inflammation. Metab Syndr Relat Disord. 2004;2:82–104. [PubMed]
9. Willerson JT, Ridker PM. Inflammation as a cardiovascular risk factor. Circulation. 2004;109 (21 Suppl 1:II2–10. [PubMed]
10. Huffman JC, Celano CM, Januzzi JL. The relationship between depression, anxiety, and cardiovascular outcomes in patients with acute coronary syndromes. Neuropsychiatr Dis Treat. 2010;6:123–136. [PMC free article] [PubMed]
11. Lamers F, van OP, Comijs HC, Smit JH, Spinhoven P, van Balkom AJ, et al. Comorbidity patterns of anxiety and depressive disorders in a large cohort study: the Netherlands Study of Depression and Anxiety (NESDA) J Clin Psychiatry. 2011;72:341–348. [PubMed]
12. Howren MB, Lamkin DM, Suls J. Associations of depression with C-reactive protein, IL-1, and IL-6: a meta-analysis. Psychosom Med. 2009;71:171–186. [PubMed]
13. Dowlati Y, Herrmann N, Swardfager W, Liu H, Sham L, Reim EK, et al. A meta-analysis of cytokines in major depression. Biol Psychiatry. 2010;67:446–457. [PubMed]
14. Pitsavos C, Panagiotakos DB, Papageorgiou C, Tsetsekou E, Soldatos C, Stefanadis C. Anxiety in relation to inflammation and coagulation markers, among healthy adults: the ATTICA study. Atherosclerosis. 2006;185:320–326. [PubMed]
15. Liukkonen T, Rasanen P, Jokelainen J, Leinonen M, Jarvelin MR, Meyer-Rochow VB, et al. The association between anxiety and C-reactive protein (CRP) levels: results from the Northern Finland 1966 birth cohort study. Eur Psychiatry. 2011;26:363–369. [PubMed]
16. Gill JM, Saligan L, Woods S, Page G. PTSD is associated with an excess of inflammatory immune activities. Perspect Psychiatr Care. 2009;45:262–277. [PubMed]
17. Spitzer C, Barnow S, Volzke H, Wallaschofski H, John U, Freyberger HJ, et al. Association of posttraumatic stress disorder with low-grade elevation of C-reactive protein: evidence from the general population. J Psychiatr Res. 2010;44:15–21. [PubMed]
18. Hoge EA, Brandstetter K, Moshier S, Pollack MH, Wong KK, Simon NM. Broad spectrum of cytokine abnormalities in panic disorder and posttraumatic stress disorder. Depress Anxiety. 2009;26:447–455. [PubMed]
19. Bankier B, Barajas J, Martinez-Rumayor A, Januzzi JL. Association between C-reactive protein and generalized anxiety disorder in stable coronary heart disease patients. Eur Heart J. 2008;29:2212–2217. [PubMed]
20. Hamer M, Gibson EL, Vuononvirta R, Williams E, Steptoe A. Inflammatory and hemostatic responses to repeated mental stress: individual stability and habituation over time. Brain Behav Immun. 2006;20:456–459. [PubMed]
21. Leonard BE, Myint A. The psychoneuroimmunology of depression. Hum Psychopharmacol. 2009;24:165–175. [PubMed]
22. Miller GE, Cohen S, Ritchey AK. Chronic psychological stress and the regulation of pro-inflammatory cytokines: a glucocorticoid-resistance model. Health Psychol. 2002;21:531–541. [PubMed]
23. Wirtz PH, von KR, Schnorpfeil P, Ehlert U, Frey K, Fischer JE. Reduced glucocorticoid sensitivity of monocyte interleukin-6 production in male industrial employees who are vitally exhausted. Psychosom Med. 2003;65:672–678. [PubMed]
24. Bauer ME. Chronic stress and immunosenescence: a review. Neuroimmunomodulation. 2008;15:241–250. [PubMed]
25. Penninx BW, Beekman AT, Smit JH, Zitman FG, Nolen WA, Spinhoven P, et al. The Netherlands Study of Depression and Anxiety (NESDA): rationale, objectives and methods. Int J Methods Psychiatr Res. 2008;17:121–140. [PubMed]
26. American Psychiatric AssociationDiagnostic and Statistical Manual of Mental Disorders4th edAmerican Psychiatric Association: Washington, DC; 2001
27. Wittchen HU. Reliability and validity studies of the WHO–Composite International Diagnostic Interview (CIDI): a critical review. J Psychiatr Res. 1994;28:57–84. [PubMed]
28. Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56:893–897. [PubMed]
29. Kabacoff RI, Segal DL, Hersen M, Van Hasselt VB. Psychometric properties and diagnostic utility of the Beck Anxiety Inventory and the State-Trait Anxiety Inventory with older adult psychiatric outpatients. J Anxiety Disord. 1997;11:33–47. [PubMed]
30. Lyketsos CG, Nestadt G, Cwi J, Heithoff K, Eaton WW. The life chart interview: a standardized method to describe the course of psychopathology. Int J Methods Psychiatric Res. 1994;4:143–155.
31. Eaton WW, Shao H, Nestadt G, Lee HB, Bienvenu OJ, Zandi P. Population-based study of first onset and chronicity in major depressive disorder. Arch Gen Psychiatry. 2008;65:513–520. [PMC free article] [PubMed]
32. Martyn KK, Belli RF. Retrospective data collection using event history calendars. Nurs Res. 2002;51:270–274. [PubMed]
33. Vogelzangs N, Duivis HE, Beekman AT, Kluft C, Neuteboom J, Hoogendijk W, et al. Association of depressive disorders, depression characteristics and antidepressant medication with inflammation. Transl Psychiatry. 2012;2:e79. [PMC free article] [PubMed]
34. Craig CL, Marshall AL, Sjostrom M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–1395. [PubMed]
35. WHO . Anatomical Therapeutic Chemical Classification. World Health Organization: Geneva; 2007. Collaborating Centre for Drug Statistics Methodology.
36. Cushman M, Legault C, Barrett-Connor E, Stefanick ML, Kessler C, Judd HL, et al. Effect of postmenopausal hormones on inflammation-sensitive proteins: the Postmenopausal Estrogen/Progestin Interventions (PEPI) Study. Circulation. 1999;100:717–722. [PubMed]
37. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:593–602. [PubMed]
38. Copeland WE, Shanahan L, Worthman C, Angold A, Costello EJ. Generalized anxiety and C-reactive protein levels: a prospective, longitudinal analysis. Psychol Med. 2012;42:2641–2650. [PMC free article] [PubMed]
39. Alexopoulos GS, Meyers BS, Young RC, Campbell S, Silbersweig D, Charlson M. ‘Vascular depression’ hypothesis. Arch Gen Psychiatry. 1997;54:915–922. [PubMed]
40. Kendler KS, Fiske A, Gardner CO, Gatz M. Delineation of two genetic pathways to major depression. Biol Psychiatry. 2009;65:808–811. [PMC free article] [PubMed]
41. Seldenrijk A, van Hout HP, van Marwijk HW, de GE, Gort J, Rustemeijer C, et al. Carotid atherosclerosis in depression and anxiety: Associations for age of depression onset. World J Biol Psychiatry. 2011;12:549–558. [PubMed]
42. Smith PJ, Blumenthal JA, Babyak MA, Doraiswamy PM, Hinderliter A, Hoffman BM, et al. Intima-media thickness and age of first depressive episode. Biol Psychol. 2009;80:361–364. [PMC free article] [PubMed]
43. You T, Nicklas BJ. Effects of exercise on adipokines and the metabolic syndrome. Curr Diab Rep. 2008;8:7–11. [PubMed]
44. Mead GE, Morley W, Campbell P, Greig CA, McMurdo M, Lawlor DA. Exercise for depression Cochrane Database Syst Rev 2009(3)CD004366. [PubMed]
45. Muller N, Schwarz MJ, Dehning S, Douhe A, Cerovecki A, Goldstein-Muller B, et al. The cyclooxygenase-2 inhibitor celecoxib has therapeutic effects in major depression: results of a double-blind, randomized, placebo controlled, add-on pilot study to reboxetine. Mol Psychiatry. 2006;11:680–684. [PubMed]

Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.

EXTRA IMPORTANT TOPIC: Back Pain Management
MORE TOPICS: EXTRA EXTRA: El Paso, TX | Chronic Pain Treatment
Post Disclaimer
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "The Connection Between Anxiety and Inflammation" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine; wellness; contributing etiological viscerosomatic disturbances within clinical presentations; associated somato-visceral reflex clinical dynamics; subluxation complexes; sensitive health issues; and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and licensure jurisdiction. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that directly or indirectly relate to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
New Mexico CNP License#: 90560, Verified
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)
(Licensed Medical Doctor)
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
Licenses and Board Certifications:
MD: Medical Doctor
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
| Yes | 363LF0000X - Nurse Practitioner - Family | NM |
90560 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
(Board Certified: Family Practice Nurse Practitioner—Multistate)*
(Licensed Nurse Practitioner & Chiropractor - Multistate)*
Clinical Director
Digital Business Card
Dr. Maria Cardenas, MD
(Board Certified: Internal Medicine)*
(Licensed Medical Doctor)*
Medical Director, Clinical Director & Collaborative Physician
NPI # 1164426749
MD License #: J2933
📆 Schedule Appointment: Schedule 24/7 (Click Here)