

Shoulder injuries are common among many athletes, however, subscapularis shoulder pain caused by injuries, although infrequent, can occasionally occur, causing complications. Direct trauma from an injury to this specific muscle-tendon structure can commonly affect overhead athletes, such as tennis players and swimmers. Generally, subscapularis shoulder pain and muscle injuries and/or conditions, which manifest in the form of weakness and inhibition, can lead to biomechanical abnormalities in the glenohumeral joint, including poor anterior stabilization of the shoulder joint in the shoulder of an individual.
Anatomy
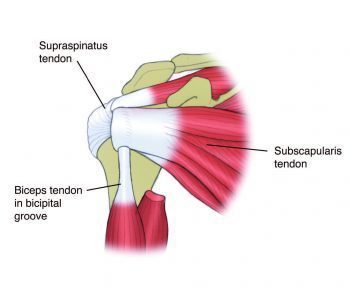
The subscapularis begins on the anterior scapular, or subscapular fossa, and introduces onto the minor tuberosity of the humerus. It is the largest of the rotator cuff muscles and its cross-sectional area is larger than the other three rotator cuff muscles combined; the infraspinatus, the teres minor and the supraspinatus. The most essential functions of the glenohumeral joint are: depressor of the humeral head; anterior stabilizer of the humeral head, which means it glides the humeral head posteriorly relative to the glenoid fossa; and internal rotator of the shoulder together with the powerful pectoralis major and latissimus dorsi.
The tendon fibres combine with the anterior capsule of the shoulder, which serve to reinforce the anterior shoulder capsule. The muscle is considered to be less substantial as a shoulder internal rotator, as the pectoralis major and latissimus dorsi are powerful internal rotators, and it’s therefore more essential as a dynamic anterior stabilizer of the glenohumeral joint due to its action in preventing anterior shear and/or glide of the humeral head.
The subscapularis has a deep connection with the long head of the biceps. This is known as a capsuloligamentous complex that functions to stabilize the long head of the biceps tendon in the bicipital groove. The pulley complex is made up of the superior glenohumeral ligament, the coracohumeral ligament, and the distal attachment of the subscapularis tendon, where it is located within the rotator interval between the anterior edge of the supraspinatus tendon and the superior edge of the subscapularis tendon. Subscapularis shoulder pain and injuries may weaken the stability of the bicep. In order to maintain the biceps tendon stabilized and in place, support of the most superior insertion point of the subscapularis from behind the ligament and tension in the superior glenohumeral ligament is needed. Issues with a biceps sling is a common cause and effect of disease in many athletes, requiring the constant and effective rotation of the shoulder, just like the cocking position during baseball pitching.
Subscapularis Shoulder Pain & Injuries
In the case of all the rotator cuff muscles, the subscapularis can be exposed to stress and pressure that may damage the muscle and its surrounding tendons. Although tears to the subscapularis are not as common as tears in the other rotator cuff, most specifically the supraspinatus, injuries causing subscapularis shoulder pain can have further complications due to its anatomical position in relation to the long head of the biceps tendon.
Isolated ruptures causing subscapularis shoulder pain have previously been recorded in the literature, Gerber and Krushell 1991. A strained hyper-extension and/or an external rotation impact on the shoulder caused by falling onto an outstretched arm, or in rare occasions, it may be an effect of a shoulder dislocation. These types of injuries will result in acute subscapularis shoulder pain along with a pain and weakness in internal rotation, increased range of movement into external rotation caused and limited by pain and a weak/pathological ‘lift-off’ test.
Direct trauma resulting in injuries to the subscapularis tendon may also result among athletes or during occupations which require a lot of powerful shoulder internal rotations, such as baseball pitching, tennis and swimming. Overusing these set of muscles and their respective tendons may develop a strain within the tendon that may not properly heal, resulting in fibrosis and fatty tissue deposition in the tendon. Trigger points in the muscle may then create muscle tightness and weakness.
Related Posts
During these cases, pain is frequently experienced as a deep anterior subscapularis shoulder pain, generally aggravated by overhead internal rotation movements, such as serving and swimming, weakness during the ‘lift-off’ test and also, reduced range of passive external rotation when the arm is placed by the side is noted.
Finally, a local muscle imbalance at the shoulder between the subscapularis and the infraspinatus may often cause issues with the position of the head of the humerus, especially where the humeral head is not in the center of the glenoid fossa and an extreme anterior shear of the humeral head can often cause an impingement along with a feeling of instability in the shoulder.
The Role of the Subscapularis for Shoulder Stability
It was previously recorded that in a forceful throwing action which used quick shoulder external rotation, individuals with shoulder injuries and/or conditions had a delayed beginning when executing the subscapularis during external rotation compared to the supraspinatus and infraspinatus. However, in normal shoulders that presented no symptoms, the subscapularis was activated earlier and before the shoulder started to externally rotate, evidence that the subscapularis works fast-forwardly to achieve movement as well as contract earlier than movement to provide anterior shoulder stability.
It is therefore suggested that individuals with subscapularis shoulder pain lose part of the functions which stabilize the shoulder, and as a result, the humeral head may glide and tear the glenohumeral joint, leading to anterior shoulder impingements.
Moreover, strength imbalances between the subscapularis and the externally rotating infraspinatus may develop complications in the glenohumeral joint. It is normal for the shoulder of an athlete to have a tight and overactive infraspinatus in relation to the subscapularis. This unevenness in the shoulder can create further issues, by which the infraspinatus tightness caused by over activity, pushes the humeral head forward in relation to the glenoid, and the weak and restricted subscapularis cannot correct this anterior shear effect. As a result, the humeral head shears forward and impinges the anterior shoulder structures, causing pain.
Clinical testing for subscapularis strength/ function
Lift-off sign
In 1991, Gerber and Krushell developed a new test for the subscapularis muscle called a lift-off test. During this test, the hand is placed on the lower back using a full shoulder internal rotation and the individual is asked to lift the hand away from the back. Not being able to perform this function may indicate weakness and/or the presence of a rupture in this muscle.
The challenge with this test is that individuals are believed to be able to perform this fully internally rotation of the arm to place the hand behind the back when, in reality, acutely injured shoulders will have difficulty performing this simple motion.

Napoleon Sign/Belly Press Sign
With this next test, the individual places their hand on the stomach with the elbow flexed 90 degrees, keeping the wrist and elbow in a straight line. The individual is then asked to press into their stomach. If the wrist flexes to compensate for the movement, the test is considered positive for a weak subscapularis.

Belly Off Sign
This test is performed by having the individual’s arm be placed in flexion and maximum IR with the elbow flexed at 90 degrees. The examiner will then hold the elbow while positioning the hand on the abdomen. The individual is advised to maintain the position while the wrist remains straight as the examiner lets go of the hand. If the hand lifts off the stomach during this process, this is indicative of a subscapularis tear. The positioning of this test is identical to the belly press sign test.
Bear Hug Test
In this particular test, the hand is placed on the opposite shoulder with the elbow anterior to the body. The examiner will then apply an external rotation force while the individual attempts to maintain the hand on the shoulder. The test is positive if the individual is unable to hold the hand on the shoulder as the examiner applies the external rotation force.

Subscapularis Strengthening
Only in rare cases does the subscapularis need direct stretching and trigger point therapy to manage tightness and other symptoms caused by over activity. It is more common for the subscapularis to need direct strengthening exercises to help control the movement of the humeral head and stabilize the humeral head into the glenoid fossa.
Below are some frequent exercises that may assist in strengthening the subscapularis.
Short Range Internal Rotation
With the arm placed in a “stop sign” position, this exercise is performed by having the individual place a band around the wrist which is attached somewhere behind the body at shoulder height. Note: the band around the wrist eliminates the tendency to flex the wrist and create movement. The individual is also instructed to touch the pectoralis major and the latissimus dorsi with the free hand to ensure that contraction in these muscles is minimized. The individual is then instructed to internally rotate the shoulder only a few degrees. This can be performed as a quick back and forth movement. The individual can work on multiple sets of a few repetitions, about 10 sets of 10 repetitions.

The arm can also be placed in a forward flexed position with the elbow in front of the shoulder. This provides an alternative joint angle for the subscapularis to work through. This exercise is performed in a similar manner to the “stop sign” position.

Belly Press Exercises
This is a similar exercise as described in the belly press test. Again the individual’s opposite hand is used to touch the pec major and latissimus dorsi. The band is again placed around the wrist not held in the hand. The individual then performs small range internal rotation movements similar to the short range exercise described as above, about 10 sets of 10 repetitions.


Iso-integration of Subscapularis into Pushing Movements
These exercise are made to accommodate the isolated contraction of the subscapularis into a functional movement such as shoulder press and/or bench press. A band or cable is held in the hand so that the direction of pull has an external rotation direction on the shoulder. The subscapularis will then need to contract to prevent the external rotation from occurring.
The individual should subsequently perform the general pressing movement of a shoulder bench press while holding the cable or tubing. The individual may perform the standard three sets of 10 repetitions while holding the band or cable.
It is important that the degree of pull from the band or cable is only minimal. If too much force is applied on the cable or there is too much tension on the band, an excessive external rotation turn is created which may engage the more powerful pec major and/or latissimus dorsi to control the external rotation twist.
Iso-integration using a dumbbell shoulder press

Iso-integration using a dumbbell bench press (start position)

Iso-integration using a dumbbell bench press (finish position)

In conclusion, research demonstrates that the subscapularis muscle plays an essential role in providing anterior glenohumeral joint stability. It’s the middle point of the humeral head along the glenoid during functional movements of the arm and  shoulder. Injuries or disorders in this muscle may lead to excessive shearing and gliding of the humeral head that may be a precursor to the more serious shoulder impingements and shoulder instabilities.
shoulder. Injuries or disorders in this muscle may lead to excessive shearing and gliding of the humeral head that may be a precursor to the more serious shoulder impingements and shoulder instabilities.
It is important for the healthcare professional to detect dysfunction in this muscle through a number of tests and direct strengthening exercises will be required to fully rehabilitate function on this muscle.
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Whole Body Wellness
Sourced through Scoop.it from: www.elpasochiropractorblog.com
By Dr. Alex Jimenez
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card