

The spine is made of bones called vertebrae, with the spinal cord running through the spinal canal in the center. The cord is made up of nerves. These nerve roots split from the cord and travel between the vertebrae into various areas of the body. When these nerve roots become pinched or damaged, the symptoms that follow are known as, radiculopathy. El Paso, TX. Chiropractor, Dr. Alexander Jimenez breaks down radiculopathies, along with their causes, symptoms and treatment.
The entire length of the spine, at each level, nerves exit through holes in the bone of the spine (foramen) on each side of the spinal column. These nerves are called nerve roots, or radicular nerves and branch out from the spine and supply different parts of the body.
Nerves exiting the cervical spine travel down through the arms, hands, and fingers. This is where neck problems affecting a cervical nerve root can cause pain, as well as, other symptoms through the arms and hands, one form of (radiculopathy). Another is low back problems that affect a lumbar nerve root. This can radiate through the leg and into the foot, another form of (radiculopathy, or sciatica), which creates leg pain and/or foot pain.
The spinal cord does not go into the lumbar spine and because the spinal canal has space in the lower back, problems in the lumbosacral region often cause nerve root problems and not a spinal cord injury. Serious conditions i.e. disc herniation or fracture in the lower back are also not likely to cause permanent loss of motor function in the legs.
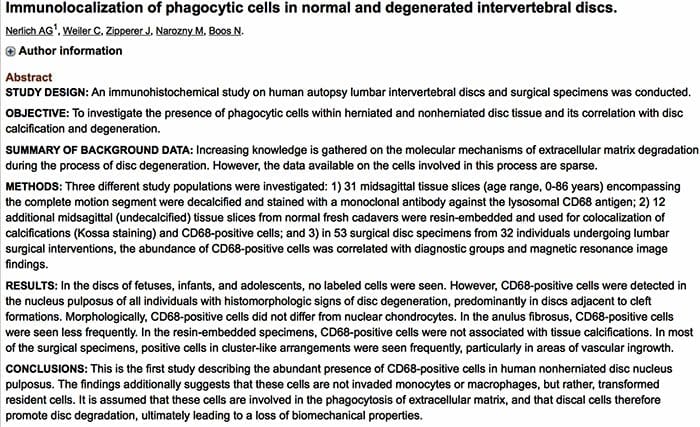
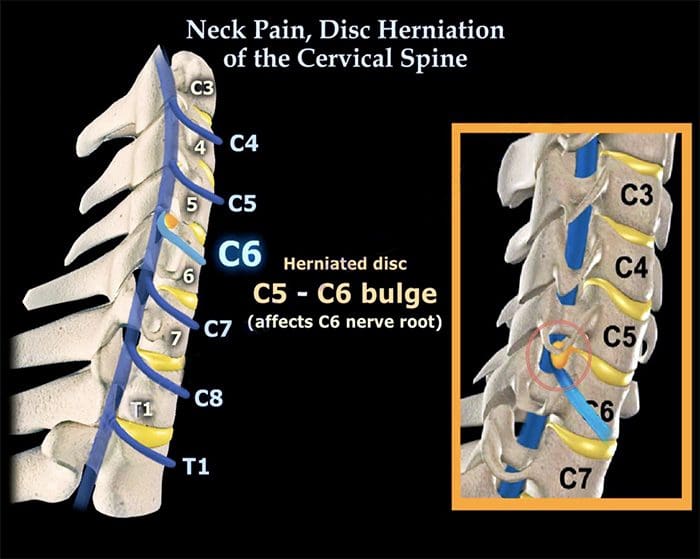
- Cervical Spine – This nerve root is named according to the Lower spinal segment that the nerve root runs between.
- Example – The nerve at C5-C6 level is called the C6 nerve root.
- It’s named like this because as it exits the spine, it passes Over the C6 pedicle (a piece of bone part of the spinal segment).
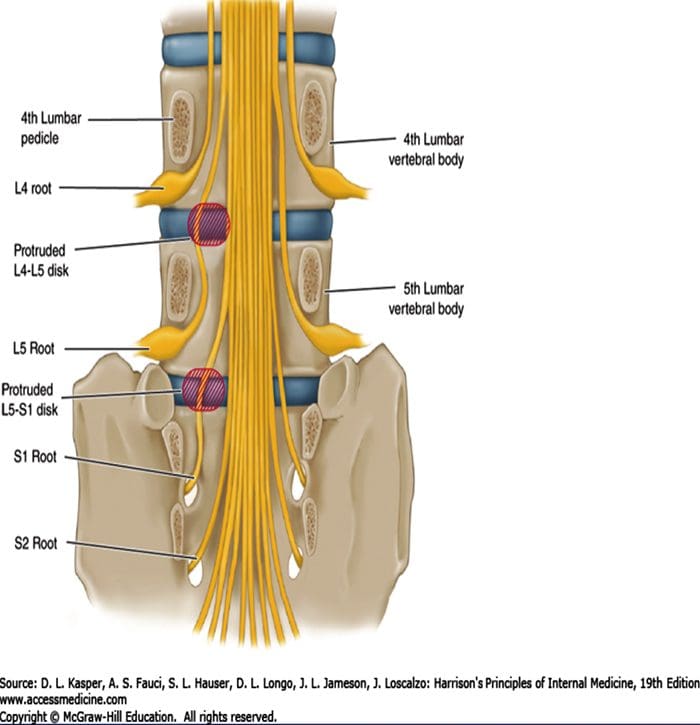
- Lumbar Spine – These nerve roots are named according to the Upper spinal segment that the nerve runs between.
- Example – The nerve at L4-L5 level is called the L4 nerve root.
- The nerve root is named this way because as it exits the spine it passes Under the L4 pedicle.
Table of Contents
Two Nerve Roots
Two nerves cross each disc level
Only one exits the spine (through the foramen) at that level.
Exiting Nerve Root – This is the nerve root exiting the spine at a certain level.
Example: L4 nerve root exits the spine at L4-L5 level.
Traversing Nerve Root – This nerve root goes across the disc and exits the spine at the level below.
Example: L5 nerve is the traversing nerve root at L4-L5 level, and is the exiting nerve root at L5-S1 level.
There is some confusion when a nerve root is compressed by disc herniation or other cause to refer both to the intervertebral level (where the disc is) and to the nerve root that is affected. This depends on where the disc herniation or protrusion is happening. It could impinge upon either the exiting nerve or the traversing nerve.
If The Traversing Nerve Is Affected
Lumbar Radiculopathy
In the lumbar spine, there is a weak area in the disc space right in front of the traversing nerve root, so lumbar discs tend to herniate or leak out and impinge on the traversing nerve.
If The Exiting Nerve Is Affected
Cervical Radiculopathy
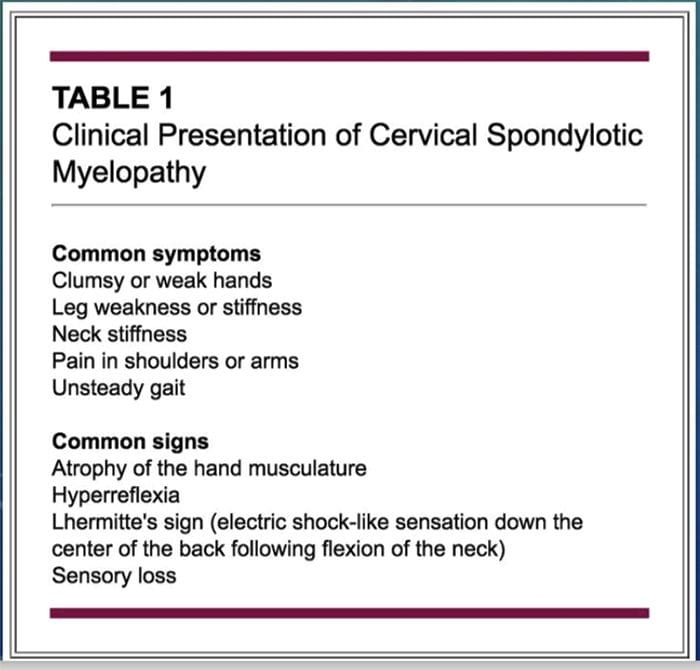
The opposite is true in the neck. In the cervical spine, the disc tends to herniate to the side, rather than toward the back and the side. If the disc material herniates to the side, it will compress or impinge the exiting nerve root.
Radiculopathy & Sciatica
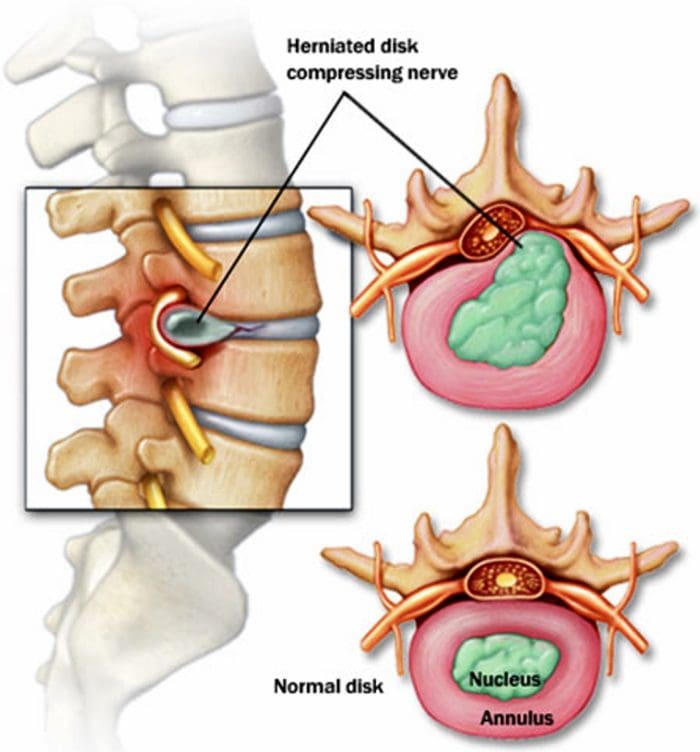
Nerve root goes by another name Radicular Nerve, and when a herniated or prolapsed disc presses on a radicular nerve, this is referred to as a radiculopathy. A medical physician might say there is herniated disc at L4-L5, which creates an L5 radiculopathy or an L4 radiculopathy. It all depends on where the disc herniation occurs (the side or the back of the disc) and which nerve is affected. And the term for radiculopathy in the low back is the ever famous Sciatica.
Radiculopathy
- A pinched nerve can occur at different areas of the spine (cervical, thoracic or lumbar).
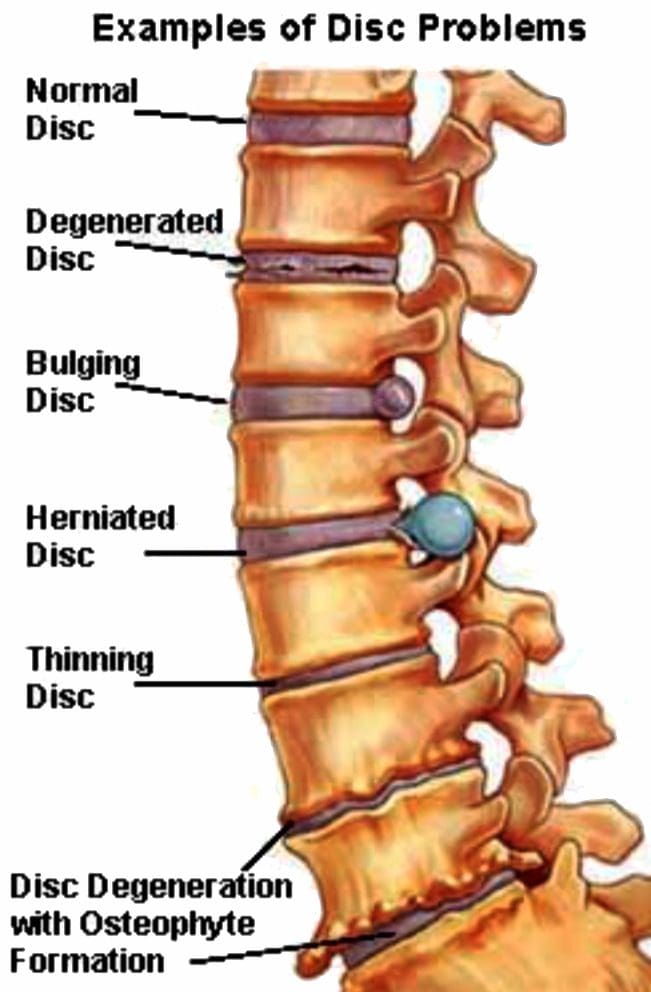
- Common causes are narrowing of the hole where the nerve roots exit, which can result from stenosis, bone spurs, disc herniation and other conditions.
- Symptoms vary but often include pain, weakness, numbness and tingling.
- Symptoms can be managed with nonsurgical treatment, but minimal surgery can also help.
Prevalence & Pathogenesis

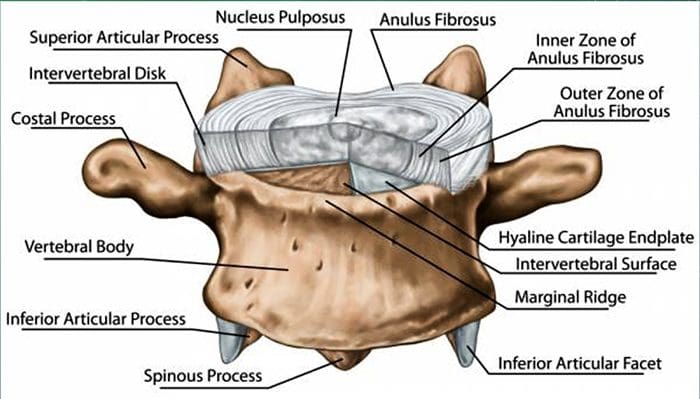
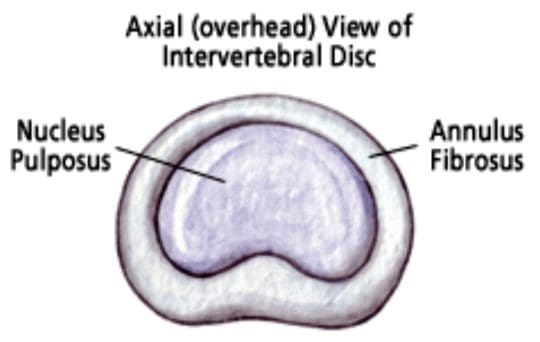
- A herniated disc can be defined as herniation of the nucleus pulposus through the fibers of the annulus fibrosus.
- Most disc ruptures occur during the third and fourth decades of life while the nucleus pulposus is still gelatinous.
- The most likely time of day associated with increased force on the disc is the morning.
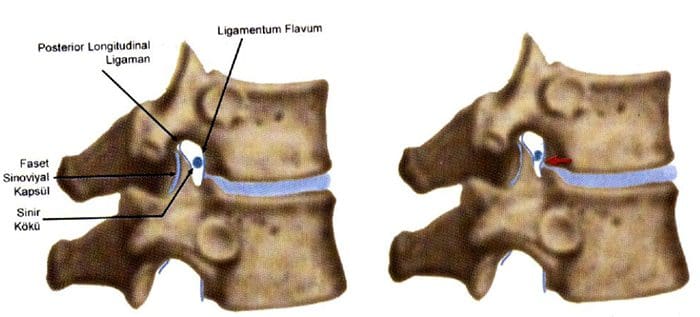
- In the lumbar region, perforations usually arise through a defect just lateral to the posterior midline, where the posterior longitudinal ligament is weakest.
 Epidemology
Epidemology
 Lumbar Spine:
Lumbar Spine:
- Symptomatic lumbar disc herniation occurs during the lifetime of approximately 2% of the general population.
- Approximately 80% of the population will experience significant back pain during the course of a herniated disc.
- The groups at greatest risk for herniation of intervertebral discs are younger individuals (mean age of 35 years)
- True sciatica actually develops in only 35% of patients with disc herniation.
- Not infrequently, sciatica develops 6 to 10 years after the onset of low back pain.
- The period of localized back pain may correspond to repeated damage to annular fibers that irritates the sinuvertebral nerve but does not result in disc herniation.
Epidemology
Cervical Spine:
- The average annual incidence of cervical radiculopathies is less than 0.1 per 1000 individuals.
- Pure soft disc herniations are less common than hard disc abnormalities (spondylosis) as a cause of radicular arm pain.
- In a study of 395 patients with nerve root abnormalities, radiculopathies occurred in the cervical and lumbar spine in 93 (24%) and 302 (76%), respectively.
Pathogenesis
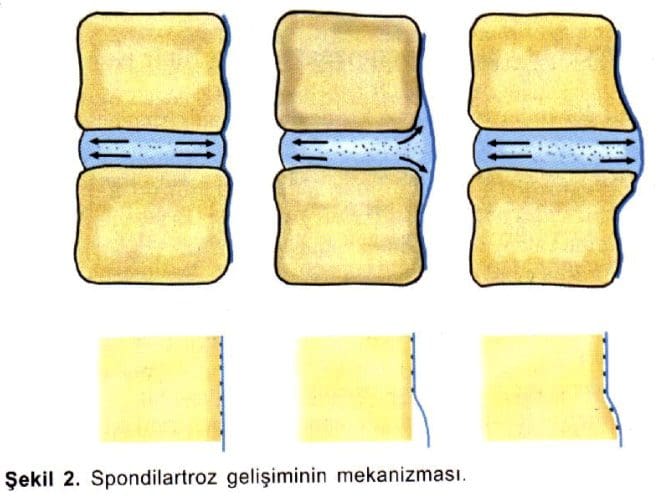
- Alterations in intervertebral disc biomechanics and biochemistry over time have a detrimental effect on disc function.
- The disc is less able to work as a spacer between vertebral bodies or as a universal joint.
Pathogenesis – LUMBAR SPINE
- The two most common levels for disc herniation are L4-L5 and L5-S1, which account for 98% of lesions; pathology can occur at L2-L3 and L3-L4 but is relatively uncommon.
Overall, 90% of disc herniations are at the L4-L5 and L5-S1 levels. - Disc herniations at L5-S1 will usually compromise the first sacral nerve root, a lesion at the L4-L5 level will most often compress the fifth lumbar root, and herniation at L3-L4 more frequently involves the fourth lumbar root.
- Disc herniation may also develop in older patients.
- Disc tissue that causes compression in elderly patients is composed of the annulus fibrosus and and portions of the cartilaginous endplate (hard disc.)
The cartilage is avulsed from the vertebral body. - Resolution of some of the compressive effects on neural structures requires resorption of the nucleus pulposus.
- Disc resorption is part of the natural healing process associated with disc herniation.
- The enhanced ability to resorb discs has the potential for resolving clinical symptoms more rapidly.
- Resorption of herniated disc material is associated with a marked increase in infiltrating macrophages and the production of matrix metalloproteinases (MMPs) 3 and 7.
- Nerlich and associates identified the origins of phagocytic cells in degenerated intervertebral discs.
- The investigation identified cells that are transformed local cells rather than invaded macrophages.
- Degenerative discs contain the cells that add to their continued dissolution.
Pathogenesis – CERVICAL SPINE
- In the early 1940s, a number of reports appeared in which cervical intervertebral disc herniation with radiculopathies was described.
- There is a direct correlation between the anatomy of the cervical spine and the location and pathophysiology of disc lesion.
- The eight cervical nerve roots exit via intervertebral foramina that are bordered anteromedially by the intervertebral disc and posterolaterally by the zygapophyseal joint.
- The foramina are largest at C2-C3 and decrease in size until C6-C7.
- The nerve root occupies 25% to 33% of the volume of the foramen.
- The C1 root exits between the occiput and the atlas (C1)
- All lower roots exit above their corresponding cervical vertebrae (the C6 root at the C5-C6 interspace), except C8, which exits between C7 and T1.
- A differential growth rate affects the relationship of the spinal cord and nerve roots and the cervical spine.

- Most acute disc herniations occur posterolaterally and in patients around the forth decade of life, when the nucleus is still gelatinous.
- The most common areas of disc herniations are C6-C7 and C5-C6.
- C7-T1 and C3-C4 disc herniations are infrequent ( less than 15 %).
- Disc herniation of C2-C3 is rare.
- Patients with upper cervical disc protrusions in the C2-C3 region have symptoms that include suboccipital pain, loss of hand dexterity, and paresthesias over the face and unilateral arm.
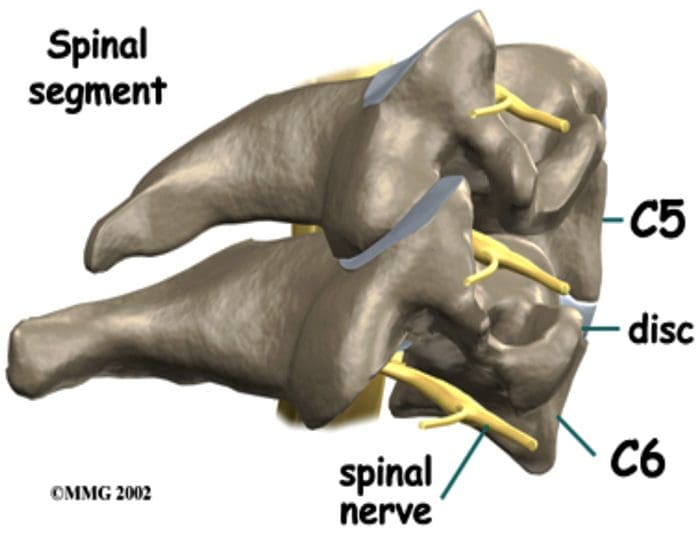
- Unlike lumbar herniated discs, cervical herniated discs may cause myelopathy in addition to radicular pain because of the anatomy of the spinal cord in the cervical region.
- The uncovertebral prominences play a role in the location of ruptured discs material.
- The uncovertebral joint tends to guide extruded disc material medially, where cord compression may also occur.
- Disc herniations usually affect the nerve root numbered most caudally for the given disc level; for example, the C3 – C4 disc affects the fourth cervical nerve root; C4- C5, the fifth cervical nerve root; C5 – C6, the sixth cervical nerve root; C6 – C7, the seventh cervical nerve root; and C7 – T1, the eighth cervical nerve root.
- Not every herniated disc is symptomatic.
- The development of symptoms depends on the reserve capacity of the spinal canal, the presence of inflammation, the size of the herniation, and the presence of concomitant disease such as osteophyte formation.
- In disc rupture, protrusion of nuclear material results in tension on the annular fibers and compress?on of the dura or nerve root causing pain.
- Also important is the smaller size of the sagittal diameter, the bony cervical spinal canal.
- Individuals in whom a cervical herniated disc causes motor dysfunction have a complication of cervical disc herniation if the spinal canal is stenotic.
Clinical History – LUMBAR SPINE
- Clinically, the patient’s major complaint is a sharp, lancinating pain.
- In many cases there may be a previous history of intermittent episodes of localized low back pain.
- The pain not only in the back but also radiates down the leg in the anatomic distribution of the affected nerve root.
- It will usually be described as deep and sharp and progressing from above downward in the involved leg.
- Its onset may be insidious or sudden and associated with a tearing or snapping sensations of the spine.
- Occasionally, when sciatica develops, the back pain may resolve because once the annulus has ruptured, it may no longer be under tension.
- Disc herniation occurs with sudden physical effort when the trunk is flexed or rotated.
- On occasion, patients with L4-L5 disc herniation have groin pain. In a study of 512 lumbar disc patients, 4.1% had groin pain.
- Finally, the sciatica may vary in intensity; it may be so severe that patients will be unable to ambulate and they will feel that their back is “locked”.
- On the other hand, the pain may be limited to a dull ache that increases in intensity with ambulation.
- Pain is worsened in the flexed position and relieved by extension of the lumbar spine.
- Characteristically, patients with herniated discs have increased pain with sitting, driving, walking, couching, sneezing, or straining.
Clinical History – CERVICAL SPINE
- Arm pain, not neck pain, is the patient’ s major complaint.
- The pain is often perceived as starting in the neck area and then radiating from this point down to shoulder, arm and forearm and usually into the hand.
- The onset of the radicular pain is often gradual, although it can be sudden and occur in association with a tearing or snapping sensation.
- As time passes, the magnitude of the arm pain clearly exceeds that of the neck or shoulder pain.
- The arm pain may also be variable in intensity and preclude any use of the arm; it may range from severe pain to a dull, cramping ache in the arm muscles.
- The pain is usually severe enough to awaken the patient at night.
- Additionally, a patient may complain of associated headaches as well as muscle spasm, which can radiate from the cervical spine to below the scapulae.
- The pain may also radiate to the chest and mimic angina (pseudoangina) or to the breast.
- Symptoms such as back pain, leg pain, leg weakness, gait disturbance, or incontinence suggest compression of the spinal cord (Myelopathy).
Physical Examination – LUMBAR SPINE
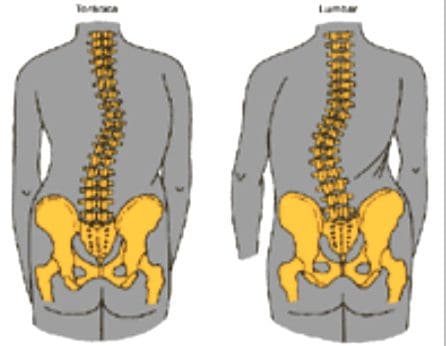
- Physical examination will demonstrated a decrease in range of motion of the lumbosacral spine, and patients may list to one side as they try to bend forward.
- The side of the disc herniation typically corresponds to the location of the scoliotic list.
- However, the specific level or degree of herniation does not correlate with the degree of list.
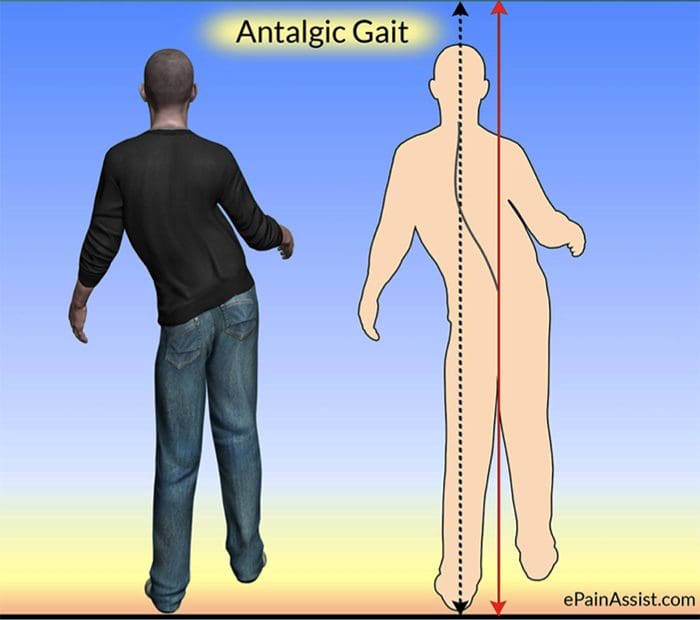
- On ambulation, patients walk with an antalgic gait in which they hold the involved leg flexed so that they put as little weight as possible on the extremity.
-
Neurologic Examination:
- The neurologic examination is very important and may yield objective evidence of nerve root compression (We should evaluate of reflex testing, muscle power, and sensation examination of the patient).
- In addition, a nerve deficit may have little temporal relevance because it may be related to a previous attack at a different level.
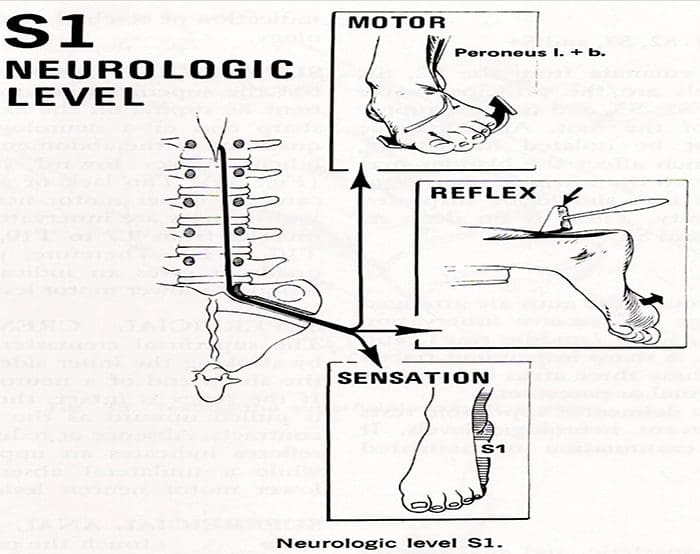
- Compression of individual spinal nerve roots results in alterations in motor, sensory, and reflex function.
- When the first sacral root is compressed, the patient may have gastrocnemius-soleus weakness and be unable to repeatedly raise up on the toes of that foot.
- Atrophy of the calf may be apperent, and the ankle (Achilles) reflex is often diminished or absent.
- Sensory loss, if present, is usually confined to the posterior aspect of the calf and the lateral side of the foot.
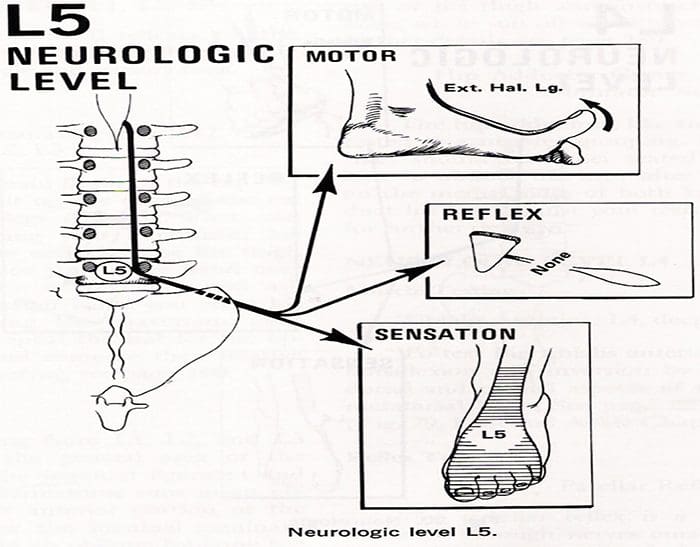
- Involvement of the fifth lumbar nerve root can lead to weakness in extension of the great toe and, in a few cases, weakness of the everters and dorsiflexors of the foot.
- A sensory deficit can appear over the anterior of the leg and the dorsomedial aspect of the foot down to the big toe
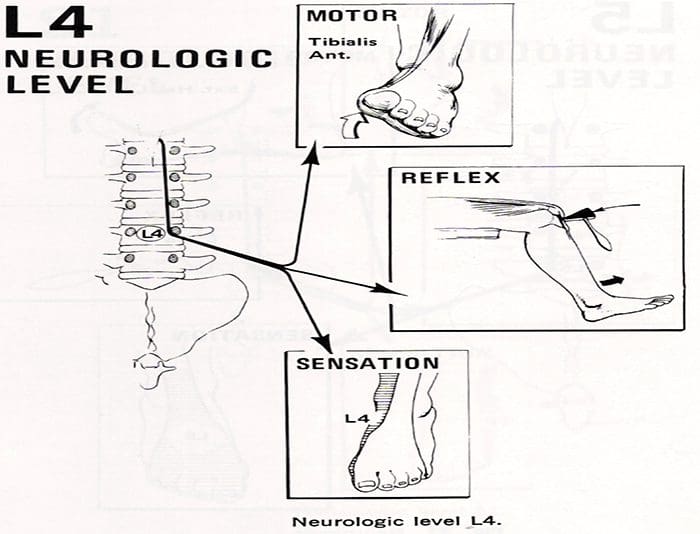
- With compression of the fourth lumbar nerve root, the quadriceps muscle is affected; the patient may note weakness in knee extension, which is often associated with instability.
- Atrophy of the thigh musculature can be marked. Sensory loss may be apparent over the anteromedial aspect of the thigh, and the patellar tendon reflex can be diminished.
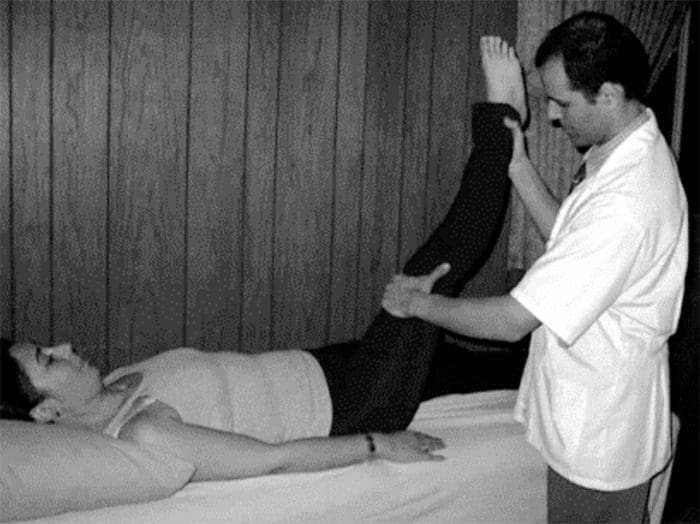
- Nerve root sensitivity can be elicited by any method that creates tension.
- The straight leg-raising (SLR)test is the one most commonly used.
- This test is performed with the patient supine.
Physical Examination – CERVICAL SPINE
Neurologic Examination:
- A neurologic examination that shows abnormalities is the most helpful aspect of the diagnostic work-up, although the examination may remain normal despite a chronic radicular pattern.
- The presence of atrophy helps document the location of the lesion, as well as its chronicity.
- The presence of subjective sensory changes is often difficult to interpret and requires a coherent and cooperative patient to be of clinical value.
- When the third cervical root is compressed, no reflex change and motor weakness can be identified.
- The pain radiates to the back of the neck and toward the mastoid process and pinna of the ear.
- Involvement of the fourth cervical nerve root leads to no readily detectable reflex changes or motor weakness.
- The pain radiates to the back of the neck and superior aspect of the scapula.
- Occasionally, the pain radiates to the anterior chest wall.
- The pain is often exacerbated by neck extension.
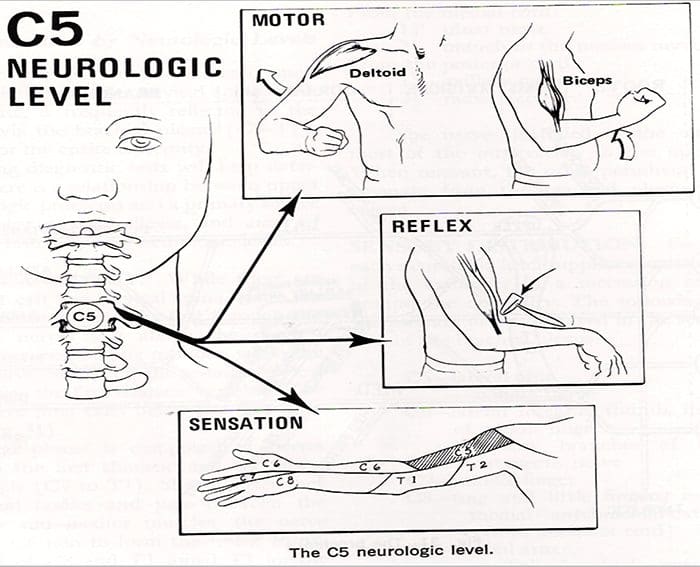
- Unlike the third and the fourth cervical nerve roots, the fifth through eighth cervical nerve roots have motor functions.
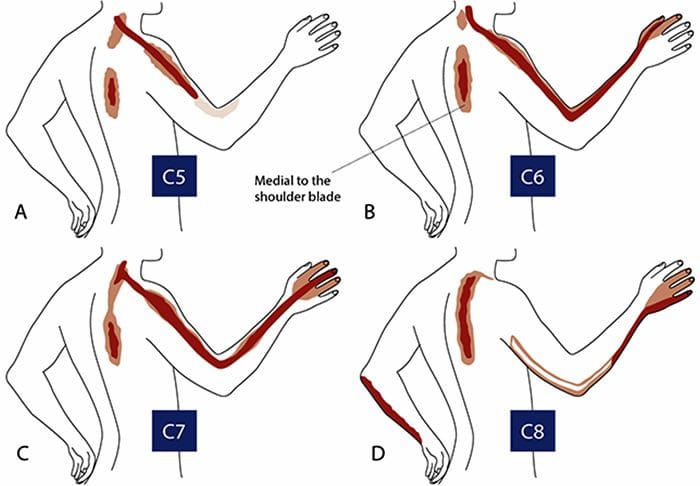
- Compression of the fifth cervical nerve root is characterized by weakness of shoulder abduction, usually above 90 degree, and weakness of shoulder extension.
- The biceps reflexes are often depressed and the pain radiates from the side of the neck to the top of the shoulder.
- Decreased sensation is often noted in the lateral aspect of the deltoid, which represents the autonomous area of the axillary nerve.
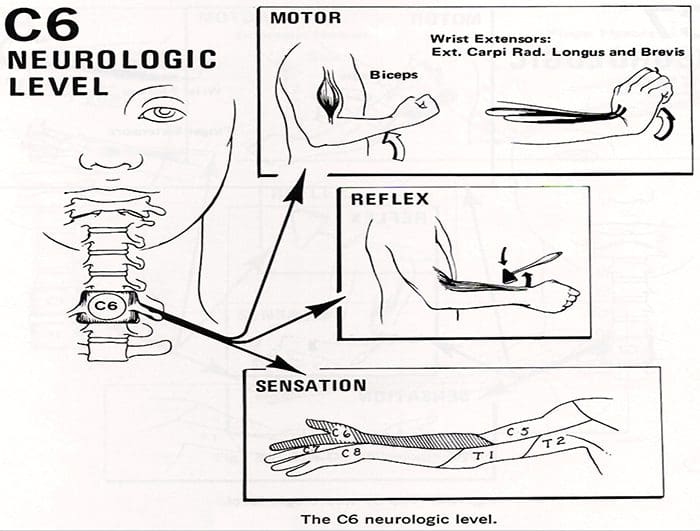
- Involvement of the sixth cervical nerve root produces biceps muscles weakness as well as diminished brachioradial reflex.
- The pain again radiates from the neck down the lateral aspect of the arm and forearm to the radial side of hand (index finger, long finger, and thumb).
- Numbness occurs occasionally in the tip of the index finger, the autonomous area of the sixth cervical nerve root.
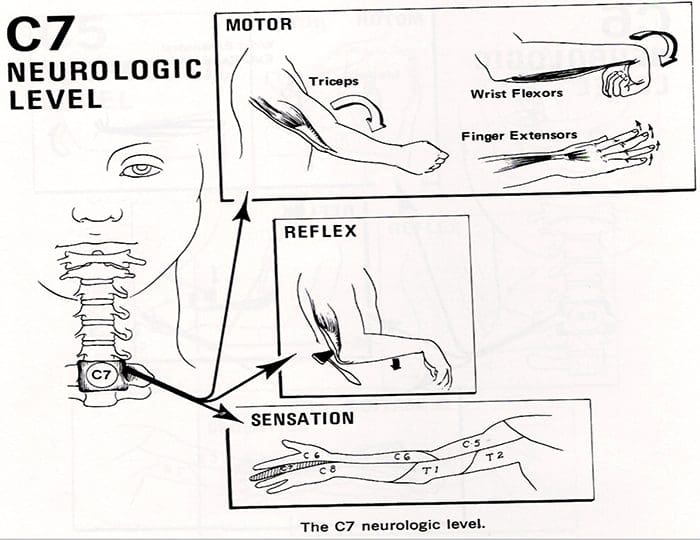
- Compression of the seventh cervical nerve root produces reflex changes in the triceps jerk test with associated loss of strength in the triceps muscles, which extend the elbow.
- The pain from this lesion radiates from the lateral aspect of the neck down the middle of the area to the middle finger.
- Sensory changes occur often in the tip of the middle finger, the autonomous area for the seventh nerve.
- Patients should also be tested for scapular winging, which may occur with C6 or C7 radiculopathies.
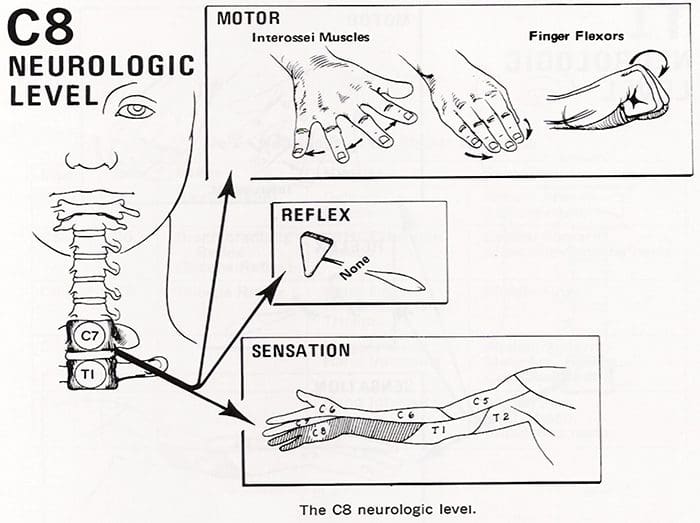
- Finally, involvement of the eighth cervical nerve root by a herniated C7-T1 disc produces significant weakness of the intrinsic musculature of the hand.
- Such involvement can lead to rapid atrophy of the interosseous muscles because of the small size of these muscles.
- Loss of the interossei leads to significant loss of fine hand motion.
- No reflexes are easily found, although the flexor carpi ulnaris reflex may be decreased.
- The radicular pain from the eighth cervical nerve root radiates to the ulnar border the hand and the ring and little fingers.
- The tip of the little finger often demonstrates diminished sensation.
- Radicular pain secondary to a herniated cervical disc may be relieved by abduction of the affected arm.
- Although these signs are helpful when present, their absence alone does not rule out a nerve root lesion.
Laboratory Data

- Medical screening laboratory test (blood counts, chemistry panels erythrocyte sedimentation rate [ESR]) are normal in patients with a herniated disc.
-
Electro diagnostic Testing
- Electromyography(EMG)is an electronic extension of the physical examination.
- The primary use of EMG is to diagnose radiculopathies in cases of questionable neurologic origin.
- EMG findings may be positive in patients with nerve root impingement.
Radiographic Evaluation – LUMBAR SPINE
- Plain x-rays may be entirely normal in a patient with signs and symptoms of nerve root impingement.
-
Computed Tomography
- Radigraphic evaluation by CT scan may demonstrate disc bulging but may not correlate with the level of nerve damage.
-
Magnetic Resonance Imaging
- MR imaging also allows visualization of soft tissues, including discs in the lumbar spine.
- Herniated discs are easily detected with MR evaluation.
- MR imaging is a sensitive technique for the detection of far lateral and anterior disc herniations.
Radiographic Evaluation – CERVICAL SPINE
-
X-rays
- Plain x-rays may be entirely normal in patients wit han acute herniated cervical disc.
- Conversely, 70% of asymptomatic women and 95% of asymptomatic men between the ages of 60 and 65 years have evidence of degenerative disc disease on plain roentgenograms.
- Views to be obtained include anteroposterior, lateral, flexion, and extension.


-
Computed Tomography
- CT permits direct visualization of compression of neural structures and is therefore more precise than myelography.
- Advantages of CT over myelography include better visualization of lateral abnormalities such as foraminal stenosis and abnormalities caudal to the myelographic block, less radiation exposure, and no hospitalization.
-
Magnetic Resonance
- MRI allows excellent visualization of soft tissues, including herniated discs in the cervical spine.
- The test is noninvasive.
- In a study of 34 patients with cervical lesions, MRI predicted 88% of the surgically proven lesions versus 81% for myelography-CT, 58% for myelography, and 50% for CT alone.
Differential Diagnosis – LUMBAR SPINE
- The initial diagnosis of a herniated disc is ordinarily made on the basis of the history and physical examination.
- Plain radiographs of the lumbosacral spine will rarely add to the diagnosis but should be obtained to help rule out other causes of pain such as infection or tumor.
- Other tests such as MR, CT, and myelography are confirmatory by nature and can be misleading when used as screening tests.
Spinal Stenosis
- Patient with spinal stenosis may also suffer from back pain that radiates to the lower extremities.
- Patients with spinal stenosis tend to be older than those in whom herniated discs develop.
- Characteristically, patients with spinal stenosis experience lower extremity pain (pseudoclaudication=neurogenic claudication) after walking for an unspecified distance.
- They also complain of pain that is exacerbated by standing or extending the spine.
- Radiographic evaluation is usually helpful in differentiating individuals with disc herniation from those with bony hypertrophy associated with spinal stenosis.
- In a study of 1,293 patients, lateral spinal stenosis and herniated intervertebral discs coexisted in 17.7% of individuals.
- Radicular pain may be caused by more than one pathologic process in an individual.
Facet Syndrome
- Facet syndrome is another cause of low back pain that may be associated with radiation of pain to structures outside the confines of the lumbosacral spine.
- Degeneration of articular structures in the facet joint causes pain to develop.
- In most circumstances, the pain is localized over the area of the affected joint and is aggravated by extension of the spine (standing).
- A deep , ill-defined, aching discomfort may also be noted in the sacroiliac joint, the buttocks, and the legs.
- The areas of sclerotome affected show the same embryonic origin as the degenerated facet joint.
- Patients with pain secondary to facet joint disease may have relief of symptoms with apophyseal injection of a long-acting local anesthetic.
- The true role of facet joint disease in the production of back and leg pain remains to be determined.
- Other mechanical causes of sciatica include congentenial abnormalites of the lumbar nerve roots, external compression of the sciatic nerve (wallet in a back pants pocket), and muscular compression of the nerve (piriformis syndrome).
- In rare circumstances, cervical or thoracic lesion should be considered if the lumbar spine is clear of abnormalities.
- Medical causes of sciatica (neural tumors or infections, for example) are usually associated with systemic symptoms in addition to nerve pain in a sciatic distribution.
Differential Diagnosis – CERVICAL SPINE
- No diagnostic criteria exist for the clinical diagnosis of a herniated cervical disc.
- The provisional diagnosis of a herniated cervical disc is made by the history and physical examination.
- The plain x-ray is usually nondiagnostic, although occasionally disc space narrowing at the suspected interspace or foraminal narrowing on oblique films is seen.
- The value of x-rays is to exclude other causes of neck and arm pain, such as infection and tumor.
- MR imaging and CT-myelography are the best confirmatory examinations for disc herniation.
- Cervical disc herniations may affect structures other than nerve roots.
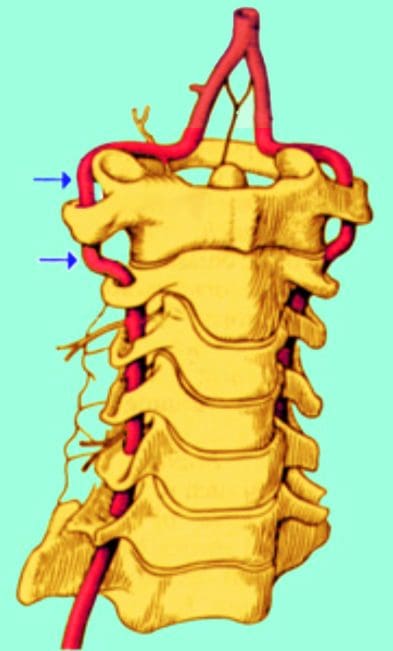
- Disc herniation may cause vessel compression (vertebral artery) associated with vertebrobasilar artery insufficiency and be manifested as blurred vision and dizziness.
- Other mechanical causes of arm pain should be excluded.
- The most common is some form of compression on a peripheral nerve.
- Such compression can occur at the elbow, forearm, or wrist. An example is compression of the median nerve by the carpal ligament leading to carpal tunnel syndrome.
- The best diagnostic test to rule out these peripheral neuropathies is EMG.
- Excessive traction on the arm secondary to heavy weights may cause radicular pain without disc compression of nerve roots.
- Spinal cord abnormalities must be considered if signs of myelopathy are present in conjunction with radiculopathies.
- Spinal cord lesions such as syringomyelia are identified by MRI, and motor neuron disease is identified by EMG.
- Multiple sclerosis should be considered in a patient with radiculopathies if the physical signs indicate lesions above the foramen magnum (optic neuritis).
- In very rare circumstances, lesions of the parietal lobe corresponding to the arm can mimic the findings of cervical radiculopathies.
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card