


Headaches are a highly common afflicting, affecting approximately 66 percent of the general population, causing pain and discomfort which alters an individual’s quality of life and work rate. Up to fourteen various forms of headaches have been previously recorded by The International Headache Society, including cervicogenic headaches. Particularly, the classification of headache disorders can be greatly beneficial when diagnosing an individual’s cause of headache.
The IHS classification of headache disorders can be categorized as follows:
The primary types of headache disorders include, headaches without a seemingly identifiable cause, for example, tension-type headaches, or TTH, migraines, chronic daily headaches, medication overuse headaches and trigeminal autonomic cephalagia, or cluster headache. The secondary types of headache disorders include, headaches associated with secondary pathologies, for example, cervicogenic headaches, TMJ, infection, brain tumors and stroke. Cranial neuropathies, facial pains and other types of headache disorders include, headaches related to neural disorders of the head and neck, for example, trigeminal neuralgia.
Since each form of headache has a different pathological foundation and because an incorrect differential diagnosis will often lead to treatment failure, it is essential to properly diagnose the type of headache. This is of particular importance for manual therapy interventions, alternatively, they are unlikely to be effective for the majority of headache forms. When considering the best clinical approach to athletes experiencing symptoms of headache, there are several helpful tools, which can be utilized when contemplating the appropriate management pathway.
Table of Contents
Function of the Trigeminocervical Nucleus (TCN)
The most common form of headaches are tension-type headaches, or TTH, affecting up to 38 percent of individuals globally, as compared to migraines, which affect up to 10 percent of the population, chronic daily headaches, affecting 3 percent and cervicogenic headaches, which affect from 2.5 to 4.1 percent of individuals. Cervicogenic headaches primarily originate as a result of musculoskeletal dysfunction in the upper three cervical sections. The prevalence is as high as 53 percent in the general population or athletes with headache symptoms after experiencing whiplash-associated trauma.
The mechanism underlying the pain involves the union between cervical and trigeminal afferent nerve fibers or vessels in the trigeminocervical nucleus, which travels down the spinal cord to the level of the vertebrae segments, C3 and C4, in the cervical spine.
The trigeminocervical nucleus has anatomical and functional progression with the dorsal grey columns of these spinal regions. For that reason, input through a sensory afferent, particularly from any of the upper three cervical nerve roots, may be incorrectly perceived as pain in the head, a concept best referred to as convergence.
Convergence between cervical afferent nerve fibers or vessels, allows for upper cervical pain to be guided to regions of the head innervated by cervical nerves, including the occipital and auricular regions. Nonetheless, combining with trigeminal afferents provides a standard guideline into the parietal, frontal, and orbital regions. This can cause confusion when diagnosing the cause of headaches.
The Different Types of Headaches
Medically distinguishing the different forms of headache can be challenging. The subjective information is absolutely crucial.
The following diagnostic criteria have been proposed by the Cervicogenic Headache International Study Group as follows:
The signs and symptoms of neck involvement as a cause of headaches includes the precipitation of headache by neck movement, postural changes and/or pressure over the upper cervical/occipital region, along with the restriction of neck range of motion, or ROM and the presence of ipsilateral neck, shoulder or vague arm pain.
Head pain characteristics are described as moderate to severe, non-throbbing and non-clustering, starting in the neck and spreading to the head. These can have a varying duration and generally last longer than a migraine headache with a long-term fluctuating pattern, becoming continuous when chronic. As for migraines, these can occur most frequently on females, identified by symptoms of nausea, photophobia and throbbing pain, following a crescendo pattern.
Diagnosis is based on these subjective features as well as a physical examination of articular, neural, and myogenic systems while understanding the mechanisms of the symptoms. Exclusion of red and yellow flags at this stage is also essential. There can be many structural causes of cervicogenic headaches.
The potential causes of cervicogenic headaches includes: psychosocial co-morbidities, such as depression and anxiety, along with reported dysfunction in the joints, muscles, neural tissues, vascular structures and others such as damage or injury to the temporomandibular joint.
Assessing Cervicogenic Headaches
The goal of the assessment is to reproduce the pain of headache from the structures surrounding the cervical spine with evidence of an associated dysfunction. By assessing the articular, neural, and muscular structures during the evaluation, one can be certain that the source of the individual’s cervicogenic headaches can be found. Subsequently, if pain cannot be reproduced, then the involvement of the cervical spine can be dismissed and other causes of headaches will need further evaluation.
The prevalence of neural tissue pain disorders has been proclaimed among 7 to 10 percent of individuals with cervicogenic headaches. In this case, pain reproduction can be used as a tool to distinguish neural tissue involvement when evaluating posture, upper cervical active range of motion, neural provocation tests combined with upper cervical range of motion, nerve palpation and neurological examination. In the same manner, if the presence of vascular involvement is suspected, a clinical framework can be suggested to allow an accurate guideline for assessment and management, primarily focusing on the diagnosis and treatment of cervicogenic headaches with articular cause.
Trauma involving forced cervical flexion, rotation, or side flexion is very common in sports and physical activities. Similar to testing ligament stability in the knee joint following trauma, screening for craniovertebral instability should be prevalent in the assessment. The following assessment tests can be used to determine the presence of cervicogenic headaches.
The Sharp Purser (Transverse Ligament) Test
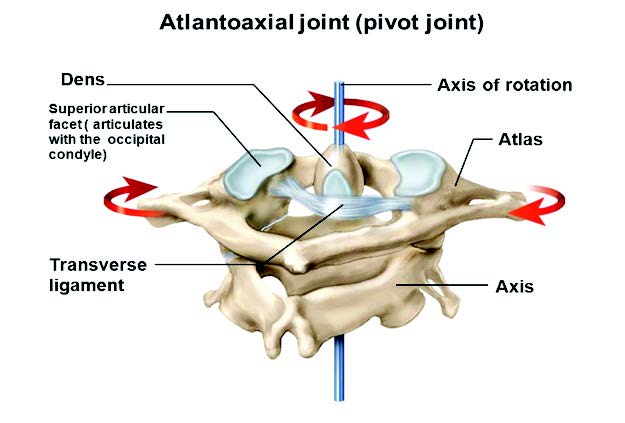
When screening for craniovertebral instability, its important to note that these tests are appropriate for diagnosing cervical instability. Healthcare professionals must be aware that other cervical-related issues can cause pain and should assess these accordingly, such as facet joint disorders.

With the individual in a sitting position, the base of the index finger is placed over the C2 spinous process. The upper cervical spine is flexed. An attempt is made to translate the individual’s head posteriorly with the C2 fixed. A positive test is a change in symptoms; a clunk sensation, and/or movement of C1 back towards the index finger on C2.
The Tectorial Membrane (Posterior Longitudinal Ligament) Test
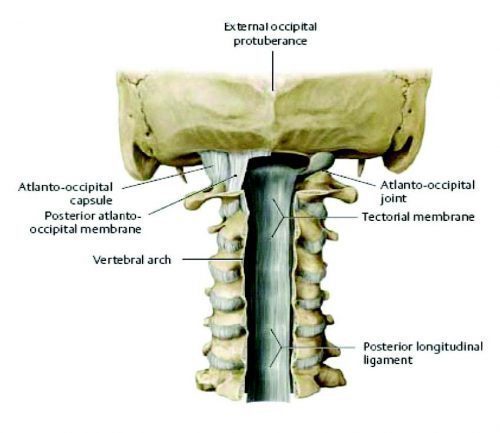
To perform this test, while the individual is sitting, a healthcare professional will craddle the occiput and head. Fixing the C2 spinous process with the base of the index finger in a downward directio. The direction of force is an axial distraction one, attempting to lift the head up on the neck to separate the two. Normal distraction should not exceed 1-2 mm.

Alar Ligament Test
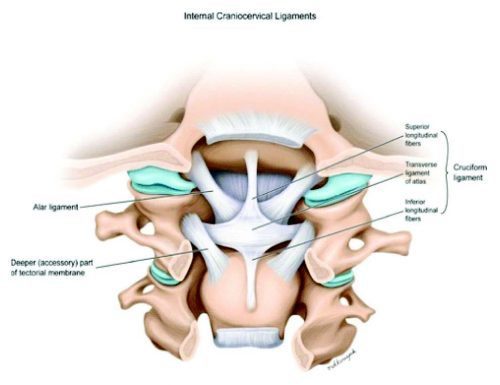
For this test, in sitting, the individual or athlete’s head will be craddled while the bific spinous process of the C2 is fixed with the index fingeer and the thumb. Side flexion down to the C2 is performed by moving the individual’s head. Any movement of the head without movement of the C2 spinous process indicates laxity of the alar ligament complex and a positive test.

Flexion/Rotation
The C1-C2 motion segments of the cervical spine accounts for 50 percent of the rotation in the cervical spine. Therefore, pain originating from an impairment of this region is a common finding in individuals with cervicogenic headaches. The flexion-rotation test, or FRT, is an easily applied clinical test developed to identify dysfunction at the C1-C2 motion segment of the spine. The Average flexion-rotation test results of the range of motion in the neck of healthy individuals is 44 degrees. The test is positive if there is pain or restriction at 10 degrees in the range of motion of the neck on either side.

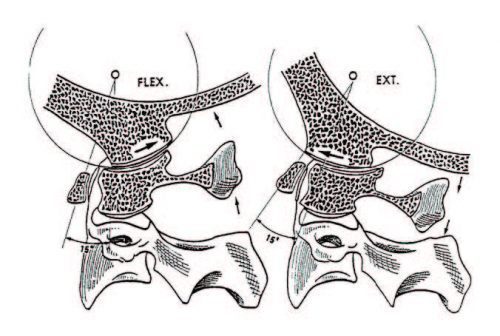
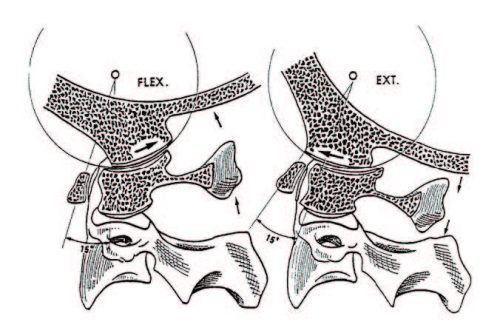
Due to the lack of intervertebral disc and altered biomechanics of the high cervical spine, combined movements are assessed differently. The primary movement available at C0-C1 is flexion and extension at 3 degrees, with the majority of movement occurring in extension at 21 degrees. Due to the sliding movement of the occipital condyles, flexion will stress the posterior capsules on the right and the left at C0-C1. The addition of ipsilateral rotation will add further pressure to the posterior capsule on the same side. This can be a nice diagnostic tool for assessing the involvement of C0-C1 as a cause for cervicogenic headaches.
CO-1 Flexion/Rotation Assessment
In order for the individual to stretch the right posterior capsule, the healthcare professional must first stand on the right of the patient and fix the mandible with their right hand while the left hand supports the occiput. Then, the specialist should retract into upper cervical flexion and add rotation using both hands. The goal is pain provocation.

In comparison, upper cervical extensions can stress the anterior capsules of the C0-C1. The addition of contra-lateral rotation will place additional pressure to the anterior capsule on the opposite side of the movement.
CO-1 Extension/Rotation Test
To stretch the right anterior capsule, the healthcare specialist must previously be standing on the right of the individual being tested, using the right elbow, the test will begin by fixing the individual’s trunk. Grasping the mandible with the right hand to control the head with the left. Protract into upper cervical extension, followed by left rotation using both hands. The goal is pain provocation.

Treating Cervicogenic Headaches
Supporting evidence has suggested that manual therapies are effective for cervicogenic headaches, specifically spinal adjustments and manipulation from qualified healthcare professionals, such as a chiropractor, including mobilization techniques with exercise. This is particularly accurate for cranio-cervical muscle strengthening and scapula positional re-training. However, further research is required to determine the effectiveness of manual therapy for headaches associated with migraines. Several effective treatments and therapy techniques for cervicogenic headaches can be utilized to relieve the symptoms of head pain as follows.
Headache Sustained Natural Apophyseal Glide (SNAG)

For a healthcare professional to perform this test, the specialist will stand by the affected individual’s side and stabilize the head with their right hand. The little finger is placed on the posterior aspect of the spinous process of C2. Horizontal pressure is applied to the little finger by the thenar eminence of the opposite hand along the upper cervical facet plane. This must be sustained for 10 seconds and repeated 6 times. Pain should be reduced during this procedure.
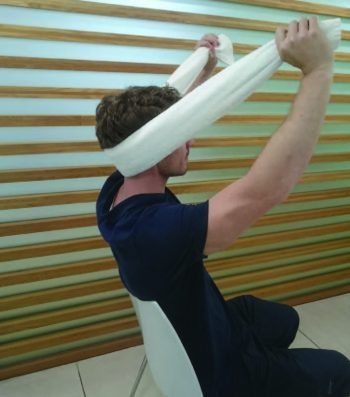
Intermittent Pain: C1-C2 Self-SNAG

If the restriction of pain occurs with a right rotation, the strap can be placed on the posterior arch of the C1 on the left side precisely below the mastoid process. The left hand will secure the strap and the right hand will pull on the strap to force rotation at the C1-C2 motion regions. Repeat this test twice, two times a day.
Intermittent Pain: C2-C3 Self-SNAG
If pain develops from below the region of the C2, then, a different form of SNAG may be utilized. In this case, the facet plane is towards the affected individual’s eyes, approximately 45 degrees. The towel edge can be used if a strap is not accessible. Sustain for 20 seconds, repeat 6 times.
Cervicogenic Headaches and Chiropractic
.video-container{position: relative; padding-bottom: 63%; padding-top: 35px; height: 0; overflow: hidden;}.video-container iframe{position: absolute; top:0; left: 0; width: 100%; height: 100%; border: none; max-width:100%!important;}
If a healthcare professional suspects trigeminocervical nucleus sensitivity, studies have demonstrated that properly managing sleep, stress and anxiety as well as following a balanced diet with moderate intensity exercise, can be beneficial for the individual’s specific type of headache. To help those affected by the dysfunction understand the concept of trigeminocervical nucleus, or TCN, sensitization, a bucket analogy can describe the concept. When the trigeminocervical nucleus is overloaded with data, this is similar to a bucket being overfilled with water. When the TCN receives too much information at once, the bucket overflows, hence, causing they symptoms of a headache. If an athlete can control the level of incoming information, they can control the level of trigeminocervical nucleus sensitization.
Treatment relies on the diagnostic criteria, but where appropriate, alternative treatment options, such as chiropractic care, can be beneficial to assess and treat headaches, including cervicogenic headaches. In particular, manual therapy has good evidence to support its foundation in treating and managing cervicogenic headaches. Chiropractic care focuses on musculoskeletal injuries and conditions, including dysfunction of the nervous system. With the use of chiropractic adjustments, a chiropractor can carefully re-align the structures of the spine, helping to reduce the pressure of the tissues as a result of irritation and swelling, ultimately improving the individual’s symptoms.
Before treatment however, the athlete should always be aware of vascular involvement and test for craniovertebral instability, particularly after trauma in specific sports and physical activities.
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card