


Low back pain, or LBP, is a very common condition which affects the lumbar spine, or the lower section of the spine. Approximately more than 3 million cases of LBP are diagnosed in the United States aline every year and about 80 percent of adults worldwide experience low back pain at some point during their lifetime. Low back pain is generally caused by injury to a muscle (strain) or ligament (sprain) or due to damage from a disease. Common causes of LBP include poor posture, lack of regular exercise, improper lifting, fracture, herniated discs and/or arthritis. Most cases of low back pain may often go away on their own, however, when LBP becomes chronic, it may be important to seek immediate medical attention. Two therapeutic methods have been utilized to improve LBP. The following article compares the effects of Pilates and McKenzie training on LBP.
Table of Contents
A Comparison of the Effects of Pilates and McKenzie Training on Pain and General Health in Men with Chronic Low Back Pain: A Randomized Trial
Abstract
- Background: Today, chronic low back pain is one of the special challenges in healthcare. There is no unique approach to treat chronic low back pain. A variety of methods are used for the treatment of low back pain, but the effects of these methods have not yet been investigated adequately.
- Aim: The aim of this study was to compare the effects of Pilates and McKenzie training on pain and general health of men with chronic low back pain.
- Materials and Methods: Thirty-six patients with chronic low back pain were chosen voluntarily and assigned to three groups of 12 each: McKenzie group, Pilates group, and control group. The Pilates group participated in 1-h exercise sessions, three sessions a week for 6 weeks. McKenzie group performed workouts 1 h a day for 20 days. The control group underwent no treatment. The general health of all participants was measured by the General Health Questionnaire 28 and pain by the McGill Pain Questionnaire.
- Results: After therapeutic exercises, there was no significant difference between Pilates and McKenzie groups in pain relief (P = 0.327). Neither of the two methods was superior over the other for pain relief. However, there was a significant difference in general health indexes between Pilates and McKenzie groups.
- Conclusion: Pilates and McKenzie training reduced pain in patients with chronic low back pain, but the Pilates training was more effective to improve general health.
- Keywords: Chronic back pain, general health, Mckenzie training, pain, Pilates training
Introduction
Low back pain with a history of more than 3 months and without any pathological symptom is called chronic low back pain. For patient with chronic low back pain, the physician should take into consideration the likelihood of muscle pain development with spinal origin, in addition to low back pain with unknown origin. This type of pain may be mechanical (increase in pain with movement or physical pressure) or nonmechanical (increase in pain at the rest time).[1] Low back pain or spine pain is the most common musculoskeletal complication.[2] About 50%–80% of healthy people may experience low back pain during their lifetime, and about 80% of the problems are related to the spine and occur in the lumbar area.[3] Low back pain may be caused by trauma, infection, tumors, etc.[4] Mechanical injuries which are caused by overuse of a natural structure, deformity of an anatomical structure, or the injury in the soft tissue are the most common reasons for back pain. From occupational health perspective, back pain is among the most important reasons for the absence from work and occupational disability;[5] in fact, the longer the period of disease,[6] the less likely it is to improve and return to work.[1] Disability due to low back pain in addition to disturbance in doing daily and social activities has a very negative effect, from social and economic perspectives, on the patient and the community, which makes chronic low back pain highly important.[3] Today, chronic low back pain is one of the critical challenges in medicine. Patients with chronic low back pain are responsible for 80% of the costs paid for the treatment of low back pain that is also the reason for mobility restrictions in most people under 45 years.[7] In the developed countries, the overall cost paid for low back pain per year is 7.1 of total share of the gross national product. Clearly, most of the cost is related to counseling and treatment of patients with chronic low back pain rather than with intermittent and recursive low back pain.[8] The existence of various methods of treatment is because of no single cause of low back pain.[9] A variety of methods such as pharmacotherapy, acupuncture, infusions, and physical methods are the most common interventions for treatment of low back pain. However, the effects of these methods remain to be fully known.[6] An exercise program, developed based on the physical conditions of patients, can promote the quality of life in patients with chronic disease.[10,11,12,13,14]


Literature shows that the effect of exercise in controlling chronic low back pain is under study and there is strong evidence about the fact that movement therapy is effective to treat low back pain.[15] However, no specific recommendations exist about the type of exercise, and the effects of certain types of movement therapies have been determined in few studies.[9] Pilates training consists of the exercises that focus on improving flexibility and strength in all the body organs, without increasing the mass of muscles or destroying them. This training method consists of controlled movements that form a physical harmony between the body and brain, and can raise the ability of the body of people at any age.[16] In addition, people who do Pilates exercise would have better sleep and less fatigue, stress, and nervousness. This training method is based on standing, sitting, and lying positions, without intervals, jumping, and leaping; thus, it may reduce injuries resulting from the joint damage because the exercise movements in the ranges of motion in the above three positions are performed with deep breathing and muscle contraction.[17] McKenzie method, also called mechanical diagnosis and therapy and based on the patient’s active participation, is used and trusted by patients and the people who use this method worldwide. This method is based on physical therapy which has been frequently studied. The distinctive characteristic of this method is the principle of initial assessment.[18] This principle is a reliable and safe method to make a diagnosis that makes the correct treatment planning possible. In this way, the time and energy are not spent for costly tests, rather McKenzie therapists, using a valid indicator, quickly recognize that how much and how this method is fruitful for the patient. More appropriately, McKenzie method is a comprehensive approach based on the correct principles whose full understanding and following is very fruitful.[19] In the recent years, non-pharmacological approaches have attracted the attention of physicians and patients with low back pain.[20] Complementary therapies[21] and treatments with holistic nature (to increase physical and mental well-being) are appropriate to manage physical illness.[13] Complementary therapies can slow down disease progression and improve capacity and physical performance. The aim of the present study is to compare the effect of the Pilates and McKenzie training on pain and general health in men with chronic low back pain.

Materials and Methods
This randomized clinical trial was conducted in Shahrekord, Iran. The total study population screened was 144. We decided to enroll at least 25% of the population, 36 individuals, using a systematic random sampling. First, the participants were numbered and a list was developed. The first case was selected using random number table and then one out of four patients was randomly enrolled. This process continued till a desired number of participants were enrolled. Then, the participants were randomly assigned to experimental (Pilates and McKenzie training) groups and control group. After explaining the research purposes to the participants, they were asked to complete the consent form for participation in the study. Furthermore, the patients were ensured that the research data are kept confidential and used only for research purposes.
Inclusion Criteria
The study population included men aged 40–55 years in Shahrekord, South-West Iran, with chronic back pain, that is, history of more than 3 months of low back pain and no specific disease or other surgery.
Exclusion Criteria
The exclusion criteria were low back arch or so-called army back, serious spinal pathology such as tumors, fractures, inflammatory diseases, previous spinal surgery, nerve root compromise in the lumbar region, spondylolysis or spondylolisthesis, spinal stenosis, neurological disorders, systemic diseases, cardiovascular diseases, and receiving other therapies simultaneously. The examiner who assessed the outcomes was blinded to group assignment. Twenty-four hours before the training, a pretest was administered to all three groups to determine pain and general health; and then, the training began after completion of the McGill Pain Questionnaire (MPQ) and the General Health Questionnaire-28 (GHQ-28). The MPQ can be used to evaluate a person experiencing significant pain. It can be used to monitor the pain over time and to determine the effectiveness of any intervention. Minimum pain score: 0 (would not be seen in a person with true pain), maximum pain score: 78, and the higher the pain score the more severe the pain. Investigators reported that the construct validity and the reliability of the MPQ were reported as a test-retest reliability of 0.70.[22] The GHQ is a self-administered screening questionnaire. Test-retest reliability has been reported to be high (0.78–0 0.9) and inter- and intra-rater reliability have both been shown to be excellent (Cronbach’s ? 0.9–0.95). High internal consistency has also been reported. The lower the score is, the better the general health is.[23]
The participants in the experimental groups started training program under supervision of a sports medicine specialist. The training program consisted of 18 sessions of supervised individual training for both groups, with the sessions held three times per week for 6 weeks. Each training session lasted for an hour and was performed at the Physiotherapy Clinic in the School of Rehabilitation of the Shahrekord University of Medical Sciences in 2014–2015. The first experimental group performed Pilates training for 6 weeks, three times a week about an hour per session. In each session, first, a 5-min warm-up and preparation procedures were run; and at the end, stretching and walking were done to return to the baseline condition. In the McKenzie group, six exercises were used: Four extension-type exercises and two flexion-types. The extension-type exercises were performed in prone and standing positions, and the flexion-type exercises in the supine and sitting positions. Each exercise was run ten times. In addition, the participants conducted twenty daily individual training sessions for an hour.[18] After training of both groups, the participants filled out the questionnaires and then the collected data were presented in both descriptive and inferential statistics. Furthermore, the control group without any training, at the end of a period when other groups have completed, filled the questionnaire. Descriptive statistics were used for central tendency indicators such as mean (± standard deviation) and relevant diagrams were used to describe the data. Inferential statistics, one-way ANOVA and post hoc Tukey’s test, were used to analyze the data. Data analysis was done by SPSS Statistics for Windows, Version 21.0 (IBM Corp. Released 2012. IBM Armonk, NY: IBM Corp). P < 0.05 was considered statistically significant.
Dr. Alex Jimenez’s Insight
Alongside the use of spinal adjustments and manual manipulations for low back pain, chiropractic care commonly utilizes therapeutic exercise methods to improve LBP symptoms, restoring the affected individual’s strength, flexibility and mobility as well as promoting a faster recovery. The Pilates and McKenzie method of training, as mentioned in the article, are compared to determine which therapeutic exercise is best for treating low back pain. As a Level I Certified Pilates Instructor, Pilates training is implemented with chiropractic treatment to improve LBP more effectively. Patients participating in a therapeutic exercise method alongside a primary form of treatment for low back pain can experience additional benefits. McKenzie training can also be implemented with chiropractic treatment to further improve LBP symptoms. The purpose of this research study is to demonstrate evidence-based information on the benefits of Pilates and McKenzie methods for low back pain as well as to educate patients on which of the two therapeutic exercises should be considered to help treat their symptoms and achieve overall health and wellness.
Level I Certified Pilates Instructors at Our Location

Results
The results showed no significant difference between the case and control groups regarding the gender, marital status, job, educational level, and income. The results showed changes in pain index and general health in the participants before and after Pilates and McKenzie training in the two experimental and even control groups [Table 1].
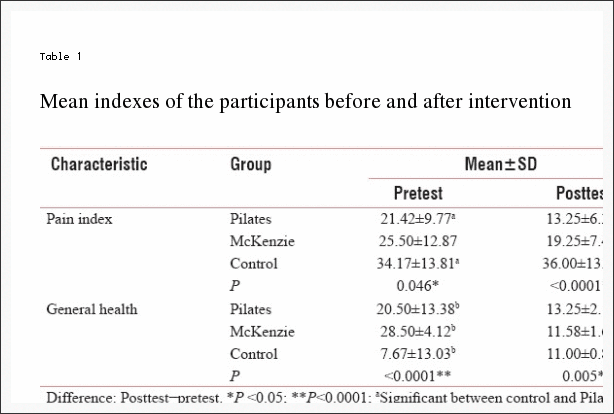
A significant difference was seen in pain and general health between the control and the two experimental groups at the pre- and post-test, so that the exercise training (both Pilates and McKenzie) resulted in reduced pain and promoted general health; while in the control group, pain increased and general health declined.
Discussion
The results of this study indicate that back pain reduced and general health enhanced after exercise therapy with both Pilates and McKenzie training, but in the control group, pain was intensified. Petersen et al. study on 360 patients with chronic low back pain concluded that at the end of 8 weeks of McKenzie training and high-intensity endurance training and 2 months training at home, pain and disability decreased in McKenzie group at the end of 2 months, but at the end of 8 months, no differences were seen among the treatments.[24]

The results of another study show that McKenzie training is a beneficial method for reducing pain and increasing the movements of the spine in patients with chronic low back pain.[18] Pilates training can be an effective method for improving general health, athletic performance, proprioception, and reduction of pain in patients with chronic low back pain.[25] The improvements in strength seen in the participants in the present study were more likely to be due to decrease in pain inhibition than to neurological changes in muscle firing/recruitment patterns or to morphological (hypertrophic) changes in the muscle. In addition, neither of the treatments was superior over the other in view of reducing the intensity of pain. In the present study, 6 weeks of McKenzie training led to significant reduction in pain levels in men with chronic low back pain. The rehabilitation of patients with chronic low back pain is aimed to restore strength, endurance, and flexibility of soft tissues.
Udermann et al. showed that McKenzie training improved pain, disability, and psychosocial variables in patients with chronic low back pain, and back stretching training did not have any additional effect on pain, disability, and psychosocial variables.[26] The results of another study show that there is a reduction in pain and disability due to McKenzie method for at least 1 week in comparison with the passive treatment in patients with low back pain, but reduction in pain and disability due to McKenzie method in comparison with the active treatment methods is desirable within 12 weeks after treatment. Overall, McKenzie treatment is more effective than passive methods to treat low back pain.[27] One of the popular exercise therapies for patients with low back pain is McKenzie training program. McKenzie method leads to improvement of low back pain symptoms such as pain in the short-term. Moreover, McKenzie therapy is more effective in comparison with passive treatments. This training is designed to mobilize the spine and to strengthen the lumbar muscles. Previous studies have shown that weakness and atrophy in the body central muscles, particularly the transverse abdominal muscle in patients with low back pain.[28] The results of this research also showed that there was a significant difference in the general health indexes between Pilates and McKenzie groups. In the present study, 6 weeks of Pilates and McKenzie training led to a significant reduction in the level of general health (physical symptoms, anxiety, social dysfunction, and depression) in men with chronic low back pain and the general health in Pilates training group improved. The results of most studies show that exercise therapy reduces pain and improves general health in patients with chronic low back pain. Importantly, the agreement about the duration, type, and intensity of the training remains to be achieved and there is no definite training program that can have the best effect on patients with chronic low back pain. Therefore, more research is needed to determine the best duration and treatment method to reduce and improve general health in patients with low back pain. In the Al-Obaidi et al. study, pain, fear, and functional disability improved after 10 weeks of treatment in patients.[5]


Besides that McKenzie training increases the range of motion of lumbar flexion. Overall, neither of the two methods of treatment was superior over the other.[18]
Borges et al. concluded that after 6 weeks of treatment, the average index of pain in experimental group was lower than the control group. Furthermore, the general health of the experimental group exhibited greater improvement than the control group. The results of this research support recommending Pilates training to patients with chronic low back pain.[29] Caldwell et al. on the university students concluded that Pilates training and Tai chi guan improved mental parameters such as self-sufficiency, quality of sleep, and morality of students but had no effect on physical performance.[30] Garcia et al. study on 148 patients with nonspecific chronic low back pain concluded that treating patients with nonspecific chronic low back pain by McKenzie training and back school caused disability to improve after treatment, but quality of life, pain, and the range of motor flexibility did not change. McKenzie treatment is typically more effective on disability than back school program.[19]
The overall findings of this study are supported by the literature, demonstrating that a Pilates program may offer a low-cost, safe alternative to the treatment of low back pain in this specific group of patients. Similar effects have been found in patients with unspecific chronic low back pain.[31]
Our study had good levels of internal and external validity and thus can guide therapists and patients considering therapies of choice for back pain. The trial included a number of features to minimize bias such as prospectively registering and following a published protocol.
Study Limitation
Small sample size enrolled in this study limits the generalization of the study findings.
Conclusion
The results of this study showed that 6-week Pilates and McKenzie training reduced pain in patients with chronic low back pain, but there was no significant difference between the effect of two therapeutic methods on pain and both exercise protocols had the same effect. In addition, Pilates and McKenzie training improved general health; however, according to the mean general health changes after the exercise therapy, it can be argued that the Pilates training has a greater effect in improving general health.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
In conclusion, when comparing the effects of Pilates and McKenzie training on general health as well as on painful symptoms in men with chronic low back pain, the evidence-based research study determined that both the Pilates and the McKenzie method of training effectively reduced pain in patients with chronic LBP. There was no significant difference between the two therapeutic methods altogether, however, the mean results of the research study demonstrated that Pilates training was more effective towards improving general health in men with chronic low back pain than McKenzie training. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
1. Bergström C, Jensen I, Hagberg J, Busch H, Bergström G. Effectiveness of different interventions using a psychosocial subgroup assignment in chronic neck and back pain patients: A 10-year follow-up. Disabil Rehabil. 2012;34:110–8. [PubMed]
2. Hoy DG, Protani M, De R, Buchbinder R. The epidemiology of neck pain. Best Pract Res Clin Rheumatol. 2010;24:783–92. [PubMed]
3. Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non-specific low back pain. Lancet. 2012;379:482–91. [PubMed]
4. Sadock BJ, Sadock VA. Kaplan and Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. New York: Lippincott Williams & Wilkins; 2011.
5. Al-Obaidi SM, Al-Sayegh NA, Ben Nakhi H, Al-Mandeel M. Evaluation of the McKenzie intervention for chronic low back pain by using selected physical and bio-behavioral outcome measures. PM R. 2011;3:637–46. [PubMed]
6. Dehkordi AH, Heydarnejad MS. Effect of booklet and combined method on parents’ awareness of children with beta-thalassemia major disorder. J Pak Med Assoc. 2008;58:485–7. [PubMed]
7. van der Wees PJ, Jamtvedt G, Rebbeck T, de Bie RA, Dekker J, Hendriks EJ. Multifaceted strategies may increase implementation of physiotherapy clinical guidelines: A systematic review. Aust J Physiother. 2008;54:233–41. [PubMed]
8. Maas ET, Juch JN, Groeneweg JG, Ostelo RW, Koes BW, Verhagen AP, et al. Cost-effectiveness of minimal interventional procedures for chronic mechanical low back pain: Design of four randomised controlled trials with an economic evaluation. BMC Musculoskelet Disord. 2012;13:260. [PMC free article] [PubMed]
9. Hernandez AM, Peterson AL. Handbook of Occupational Health and Wellness. Springer: 2012. Work-related musculoskeletal disorders and pain; pp. 63–85.
10. Hassanpour Dehkordi A, Khaledi Far A. Effect of exercise training on the quality of life and echocardiography parameter of systolic function in patients with chronic heart failure: A randomized trial. Asian J Sports Med. 2015;6:e22643. [PMC free article] [PubMed]
11. Hasanpour-Dehkordi A, Khaledi-Far A, Khaledi-Far B, Salehi-Tali S. The effect of family training and support on the quality of life and cost of hospital readmissions in congestive heart failure patients in Iran. Appl Nurs Res. 2016;31:165–9. [PubMed]
12. Hassanpour Dehkordi A. Influence of yoga and aerobics exercise on fatigue, pain and psychosocial status in patients with multiple sclerosis: A Randomized Trial. J Sports Med Phys Fitness. 2015 [Epub ahead of print] [PubMed]
13. Hassanpour-Dehkordi A, Jivad N. Comparison of regular aerobic and yoga on the quality of life in patients with multiple sclerosis. Med J Islam Repub Iran. 2014;28:141. [PMC free article] [PubMed]
14. Heydarnejad S, Dehkordi AH. The effect of an exercise program on the health-quality of life in older adults. A randomized controlled trial. Dan Med Bull. 2010;57:A4113. [PubMed]
15. van Middelkoop M, Rubinstein SM, Verhagen AP, Ostelo RW, Koes BW, van Tulder MW. Exercise therapy for chronic nonspecific low-back pain. Best Pract Res Clin Rheumatol. 2010;24:193–204. [PubMed]
16. Critchley DJ, Pierson Z, Battersby G. Effect of pilates mat exercises and conventional exercise programmes on transversus abdominis and obliquus internus abdominis activity: Pilot randomised trial. Man Ther. 2011;16:183–9. [PubMed]
17. Kloubec JA. Pilates for improvement of muscle endurance, flexibility, balance, and posture. J Strength Cond Res. 2010;24:661–7. [PubMed]
18. Hosseinifar M, Akbari A, Shahrakinasab A. The effects of McKenzie and lumbar stabilization exercises on the improvement of function and pain in patients with chronic low back pain: A randomized controlled trial. J Shahrekord Univ Med Sci. 2009;11:1–9.
19. Garcia AN, Costa Lda C, da Silva TM, Gondo FL, Cyrillo FN, Costa RA, et al. Effectiveness of back school versus McKenzie exercises in patients with chronic nonspecific low back pain: A randomized controlled trial. Phys Ther. 2013;93:729–47. [PubMed]
20. Hassanpour-Dehkordi A, Safavi P, Parvin N. Effect of methadone maintenance treatment of opioid dependent fathers on mental health and perceived family functioning of their children. Heroin Addict Relat Clin. 2016;18(3):9–14.
21. Shahbazi K, Solati K, Hasanpour-Dehkordi A. Comparison of hypnotherapy and standard medical treatment alone on quality of life in patients with irritable bowel syndrome: A Randomized Control Trial. J Clin Diagn Res. 2016;10:OC01–4. [PMC free article] [PubMed]
22. Ngamkham S, Vincent C, Finnegan L, Holden JE, Wang ZJ, Wilkie DJ. The McGill Pain Questionnaire as a multidimensional measure in people with cancer: An integrative review. Pain Manag Nurs. 2012;13:27–51. [PMC free article] [PubMed]
23. Sterling M. General health questionnaire-28 (GHQ-28) J Physiother. 2011;57:259. [PubMed]
24. Petersen T, Kryger P, Ekdahl C, Olsen S, Jacobsen S. The effect of McKenzie therapy as compared with that of intensive strengthening training for the treatment of patients with subacute or chronic low back pain: A randomized controlled trial. Spine (Phila Pa 1976) 2002;27:1702–9. [PubMed]
25. Gladwell V, Head S, Haggar M, Beneke R. Does a program of pilates improve chronic non-specific low back pain? J Sport Rehabil. 2006;15:338–50.
26. Udermann BE, Mayer JM, Donelson RG, Graves JE, Murray SR. Combining lumbar extension training with McKenzie therapy: Effects on pain, disability, and psychosocial functioning in chronic low back pain patients. Gundersen Lutheran Med J. 2004;3:7–12.
27. Machado LA, Maher CG, Herbert RD, Clare H, McAuley JH. The effectiveness of the McKenzie method in addition to first-line care for acute low back pain: A randomized controlled trial. BMC Med. 2010;8:10. [PMC free article] [PubMed]
28. Kilpikoski S. The McKenzie Method in Assessing, Classifying and Treating Non-Specific Low Back Pain in Adults with Special Reference to the Centralization Phenomenon. Jyväskylä University of Jyväskylä 2010
29. Borges J, Baptista AF, Santana N, Souza I, Kruschewsky RA, Galvão-Castro B, et al. Pilates exercises improve low back pain and quality of life in patients with HTLV-1 virus: A randomized crossover clinical trial. J Bodyw Mov Ther. 2014;18:68–74. [PubMed]
30. Caldwell K, Harrison M, Adams M, Triplett NT. Effect of pilates and taiji quan training on self-efficacy, sleep quality, mood, and physical performance of college students. J Bodyw Mov Ther. 2009;13:155–63. [PubMed]
31. Altan L, Korkmaz N, Bingol U, Gunay B. Effect of pilates training on people with fibromyalgia syndrome: A pilot study. Arch Phys Med Rehabil. 2009;90:1983–8. [PubMed]

Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.

IMPORTANT TOPIC: EXTRA EXTRA: Treating Sciatica Pain
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card