

In this article chiropractor Dr. Alexander Jimenez focuses on neck injury management and rehabilitation, with the aim of a return to complete performance.
Clinicians can hopefully find the merit in checking the cervical spine’s competency when screening and monitoring
especially in sports in which athletes are at risk of neck injuries as a result of axial loading, prolonged posture exposure, whiplash and external forces like vibrations and G force.
This article looks at treatment strategies that can be applied to all or any neck dysfunctions from acute injuries, right through to getting athletes back in their performance environment in peak condition. As with all injury management procedures, there has to be a very clear understanding of the injury and planned rehabilitation, with the athlete
and higher performance team/coaches etc.. For the sake of simplicity, we’ll break this rehabilitation down into four phases:
- Early management
- Initial rehabilitation
- Rehabilitation progression
- Return to performance.
Table of Contents
Early Management
This stage of rehabilitation should begin as soon as any severe cervical or head injury has been excluded after thorough medical assessment and additional investigation if appropriate. The key goals in early management following neck trauma are reduction of irritation, loss of muscle spasm and restoration of normal range of movement.
High quality evidence on the management of severe cervical pain is missing. This should be combined with postural education and ensuring that there aren’t compensatory dysfunctions across the rest of the kinetic chain, particularly the shoulder girdle, thoracic and lumbar spine.
The Initial therapy should be carried out together with the neck in neutral alignment along with also a ‘gravity-eliminated’ position to decrease any nerve root, disc or facet joint irritation and limit involvement of over active superficial muscles.
Gentle selection of motion has great immediately and is carried out using the periods as explained by Jull et al. (2008) in the ‘Cranio-Cervical Flexion Evaluation’ (see article component I) with a pressure cuff for feedback and working through progressive pressure increases and maintains(4). Once the athlete could achieve this, avoiding compensation strategies, the routine ought to be accomplished independently regularly throughout the day, and also may be progressed to more gravity challenging and sport certain positions.
Following the decrease in acute Symptoms, the restoration of cervical movement in all planes necessary for the
athlete’s specific sport, and also the ability to trigger and keep deep neck flexors, the athlete may progress to ‘first
rehabilitation’
Initial Rehabilitation
This phase of rehabilitation is predominant In Building neck mobilizer strength without undermining the musculature to
excessive forces. Monitoring and screening information should be utilized where available to aid programming. Full selection of movement and DNF fortifying should continue during this stage.
Commonly, when managing peripheral For instance, in the game of Skeleton, the Athlete needs to maintain neck posture in prone on the sled. Motorcyclists must keep neck posture while on a motorcycle, therefore need to have their balance challenged alongside reinforcing. It’s also important to think about any helmets or headgear that’s worn as this may also be introduced at this stage.
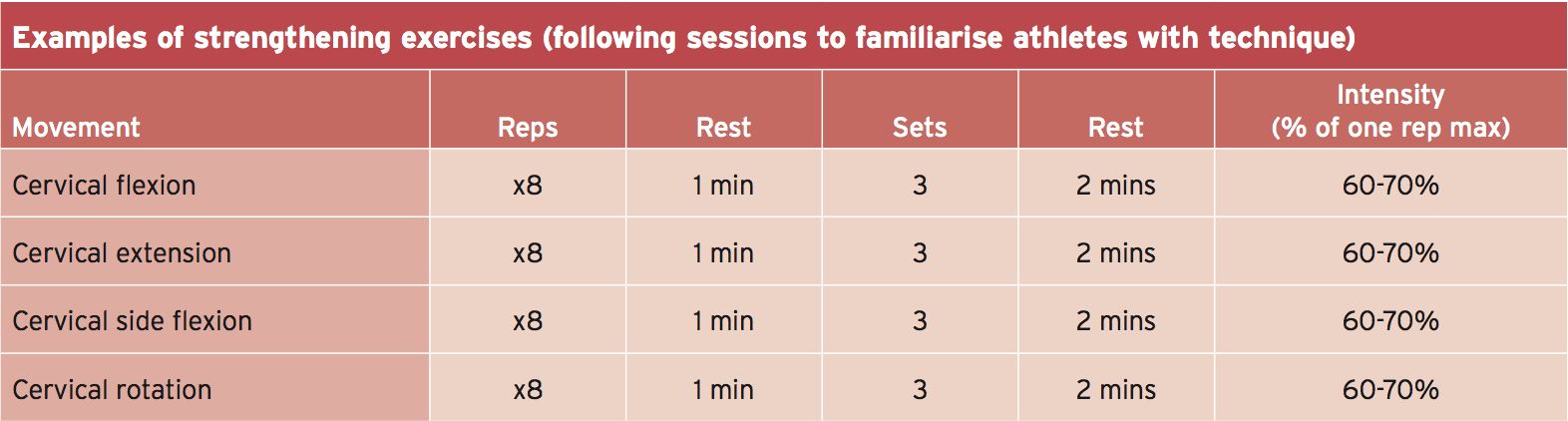
First strength training should start at A medium volume and low intensity and be gradually increased concerning repetition, length of contraction and sets. As during examination, considerations should be made to stabilize the chest and detoxify lower limb involvement so as to guarantee true neck fortifying.
Rehabilitation Progression
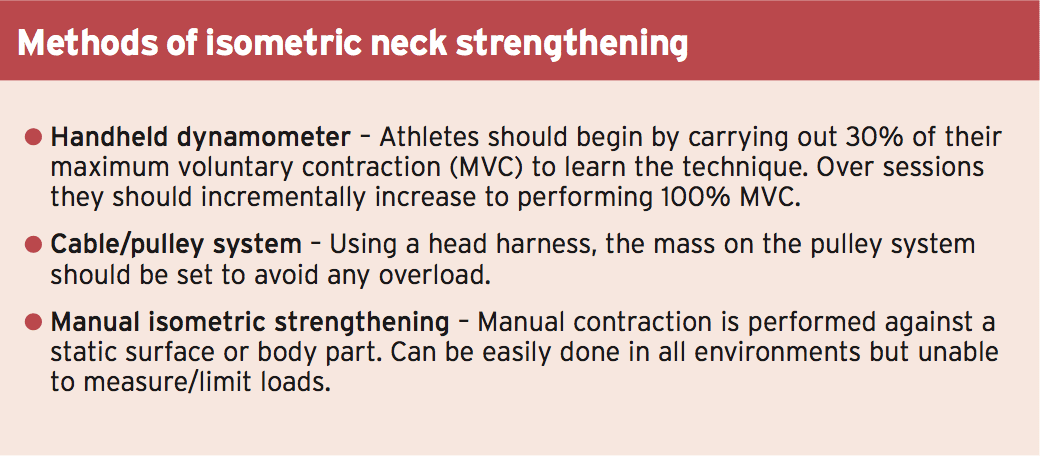
Once asymptomatic, and if isometric Contraction of 100% MVC and full selection of motion was achieved, the concentrate should advance to eccentric and concentric neck strengthening through scope. This is commonly a region that is recognized as a weakness through screening and so can be used in athlete development as well as return from injury.
The athlete’s background ought to be For instance, rugby players will probably likely to have considerable more exposure to throat strength training formerly than a young gymnast returning from injury.
Through-range strengthening should be Higher volume and medium intensity, and should be carried out using manual or dynamometry opposition. Initially cable machines can lead to overload but they are sometimes applied as a growth. Movements should begin from the sagittal plane and incorporate coronal and transverse plane strength.
Principles of overload should be maintained with neck strengthening; small gains should be expected to occur gradually rather than seeing abrupt spikes in training. This is especially important if understanding the body and the demand for the stability across several small joints.
Once baseline strength was recovered, sport specific neck training can begin. In contact sports, tackle bags can be used to duplicate controlled contact. Divers may return to low board dives and drivers to simulation work. If athletes are subjected to outside forces such as G vibration and force, this too needs to be duplicated as rehabilitation and injury prevention.
 If the athlete remains pain free, has Strength comparable to baseline measures, does not have any change in shoulder or back kinematics, and has participated in controlled normal training situations (like additional external forces) then the athlete can progress to ‘return to performance’.
If the athlete remains pain free, has Strength comparable to baseline measures, does not have any change in shoulder or back kinematics, and has participated in controlled normal training situations (like additional external forces) then the athlete can progress to ‘return to performance’.
Return To Performance
The last stage of rehabilitation in the neck Injury combines the strength training the athlete has honed, with an emphasis on the restoration of specific skills required to return for their own particular sport, together with regaining confidence in being exposed to forces on the cervical spine.
Incorporating the aspect of Unanticipated load is crucial at this point. This training mode should be practiced in rugby prior to going into a contested scrum situation, prior to heading a soccer, and when tumbling in gymnastics. By combining training procedures like isometric, isokinetic strengthening, exposure to changes and vibration in and out of the game special setting, there’s a heightened likelihood of adapting neural elements resulting in optimal motor ability, muscular control and co-ordination.
As with any harm, return-to- Performance programming is injury and athlete specific. As such, the conclusions resulting in return to perform should be centered on the individual athlete but involve the entire interdisciplinary team. The athlete should be physically and psychologically prepared to return with strength, confidence and skill shortages addressed in order to reduce risk of further harm and maximize the individual’s operation on return.
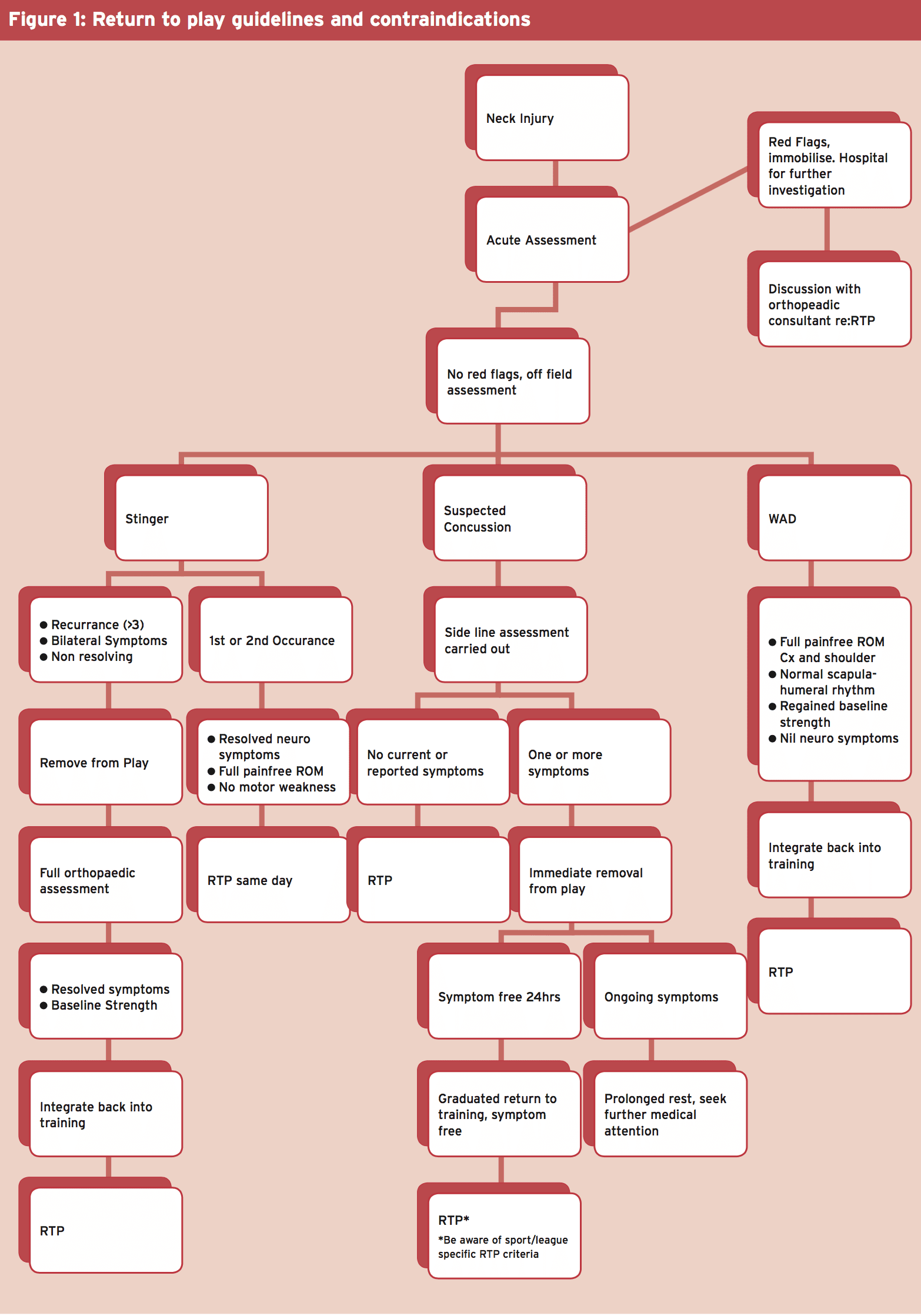
Return to performance (RTP) protocols Will change depending on injury, sport and position the athlete is returning to. Figure 1 summarizes the available evidence for a guide to key contraindications when coming to perform following common neck injuries.
 The timing of post-injury neck training Should be carefully considered when programming as part of a strengthening regimen; neck fortifying is recognized to be fatiguing and strength is originally reduced for up to a day post loading (likely longer in females)(6). Therefore, heavy neck-strength training followed by return to performance in quick succession should be avoided to minimize the possibility of further harm.
The timing of post-injury neck training Should be carefully considered when programming as part of a strengthening regimen; neck fortifying is recognized to be fatiguing and strength is originally reduced for up to a day post loading (likely longer in females)(6). Therefore, heavy neck-strength training followed by return to performance in quick succession should be avoided to minimize the possibility of further harm.
Sports with heavier programs and much less This must also be an important reason to check the athlete performing under varying amounts of exhaustion, and be sure they are strong enough to resist the forces they’re exposed to while contending.
Summary
All neck weakness and movement Dysfunctions discovered through assessment and screening ought to be addressed immediately in order to avoid additional injury. Rehabilitation should progress from regaining range of motion, strengthening the neck and surrounding structures, to sport specific coaching. Deep understanding of sport specific demands and loads that the neck is exposed to is crucial for practitioners to deliver optimal rehabilitation. This can be aided by the use Of baseline data and ongoing research to the region. By following a very clear assessment and rehabilitation therapy specific to individuals, we can minimize further injury and make sure athletes are returning to optimal performance with the particular strength and movement characteristics required.
References
1. Conservative treatments for whiplash. Cochrane Database of Systematic Reviews 2007
2. Advances in Physiotherapy 2006; 8(98-105)
3. Sports Medicine 2009. 39(9): 697-7
4. Journal of Manipulative and Physiological Therapeutics 2008. 31:525-533
5. American Journal of Sports Medicine 2004. 42:566
6. Physical Therapy in Sport 2010. 11(3):75-80
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card