

Mechanoreceptive Pain: According to the CDC, “more than 50% of U.S. adults (125 million) had a musculoskeletal pain disorder in 2012.”
“More than 40% of adults with a musculoskeletal pain disorder used a complementary health approach for any reason in 2012. This was significantly higher than use among persons without a musculoskeletal pain disorder (24.1%). Use of complementary health approaches for any reason among persons with neck pain or problems was more than twice as high as use among persons without these problems.”
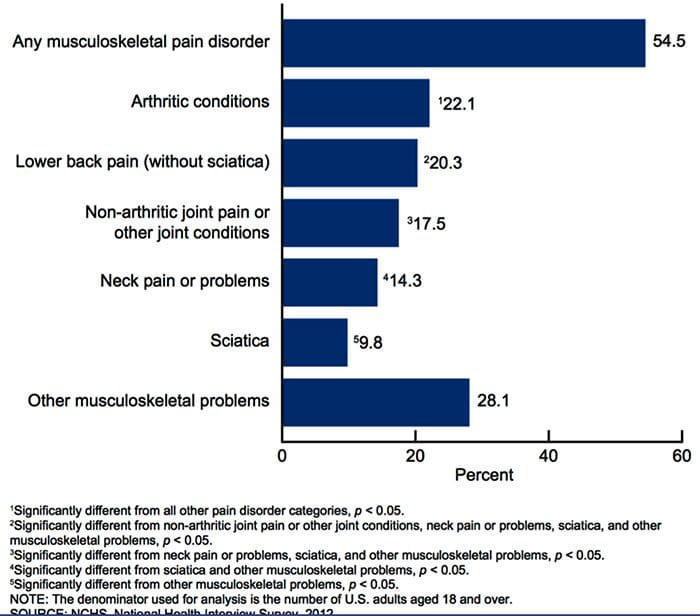
Retrieved from: https://www.cdc.gov/nchs/data/nhsr/nhsr098.pdf
Table of Contents
UNDERSTANDING PAIN IS IMPORTANT
“Among adults with a musculoskeletal pain disorder, use of any complementary health approach was highest among those with neck pain or problems (50.6%), followed by persons with other musculoskeletal problems (46.2%).”
“Use of complementary health approaches for any reason among persons with neck pain or problems was more than twice as high as use among persons without these problems.”
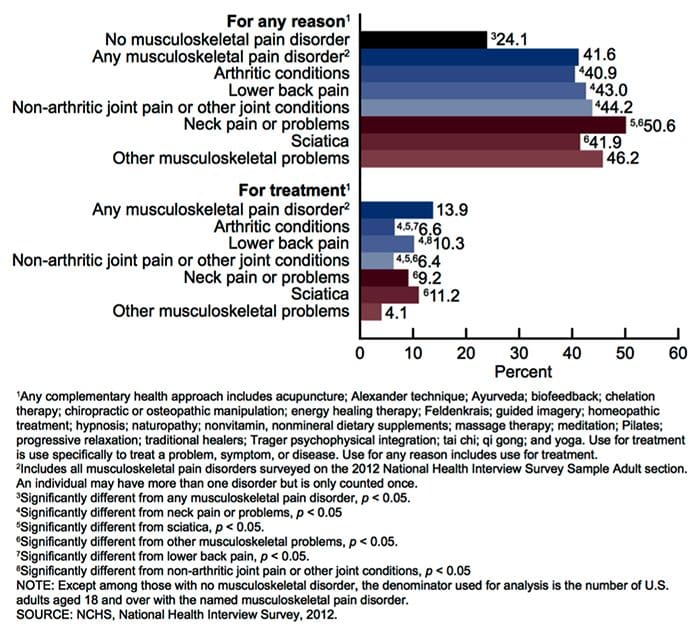
Retrieved from: https://www.cdc.gov/nchs/data/nhsr/nhsr098.pdf
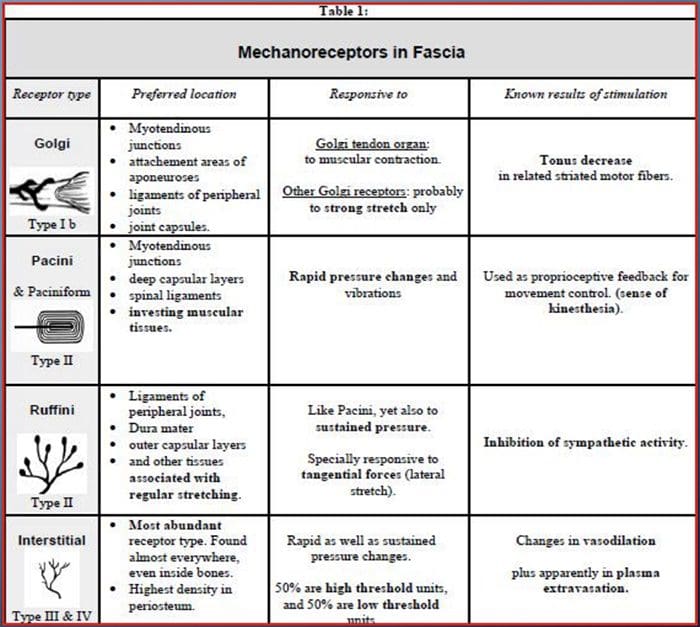
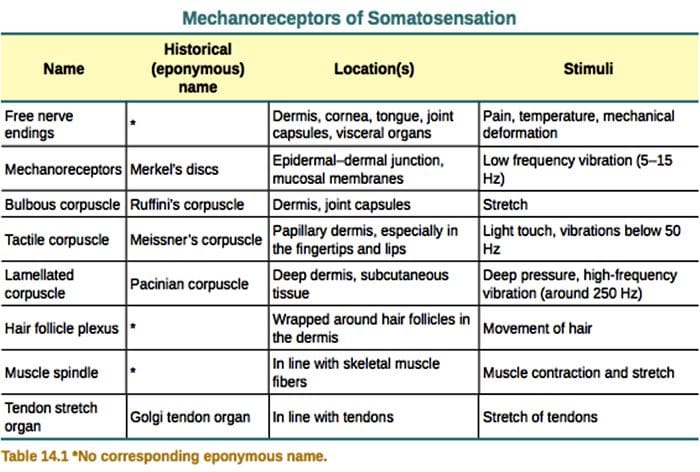
WHAT IS A MECHANORECEPTOR?
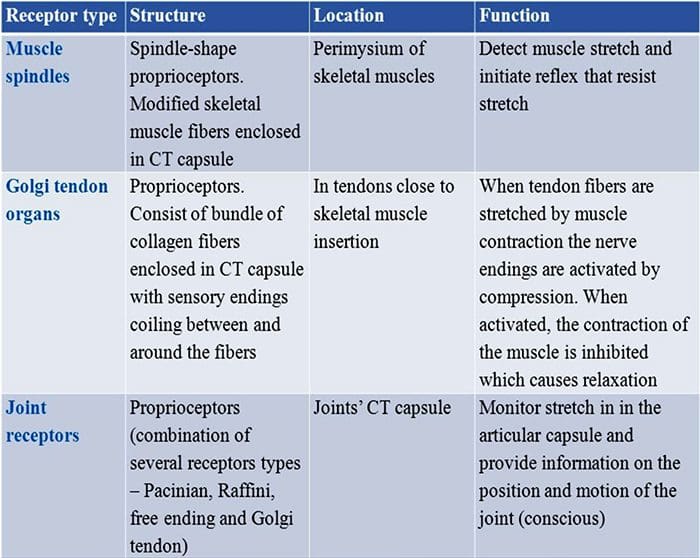
- Mechanoreceptors are sensory receptors that respond to mechanical pressure or distortion.
- These include cutaneous receptors for touch, receptors that monitor muscle length and tension, auditory and vestibular receptors and others.
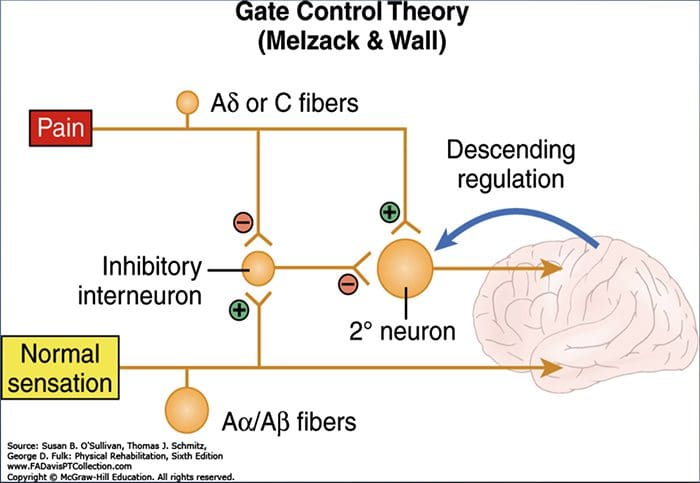
 GATE CONTROL THEORY OF PAIN
GATE CONTROL THEORY OF PAIN
- Non-painful input closes the gates to painful input.
- This prevents pain sensations from traveling to higher cortical levels
- Small diameter afferents (pain) impede inhibition of pain
- Large diameter afferents (vibration) tend to excite inhibition of pain.
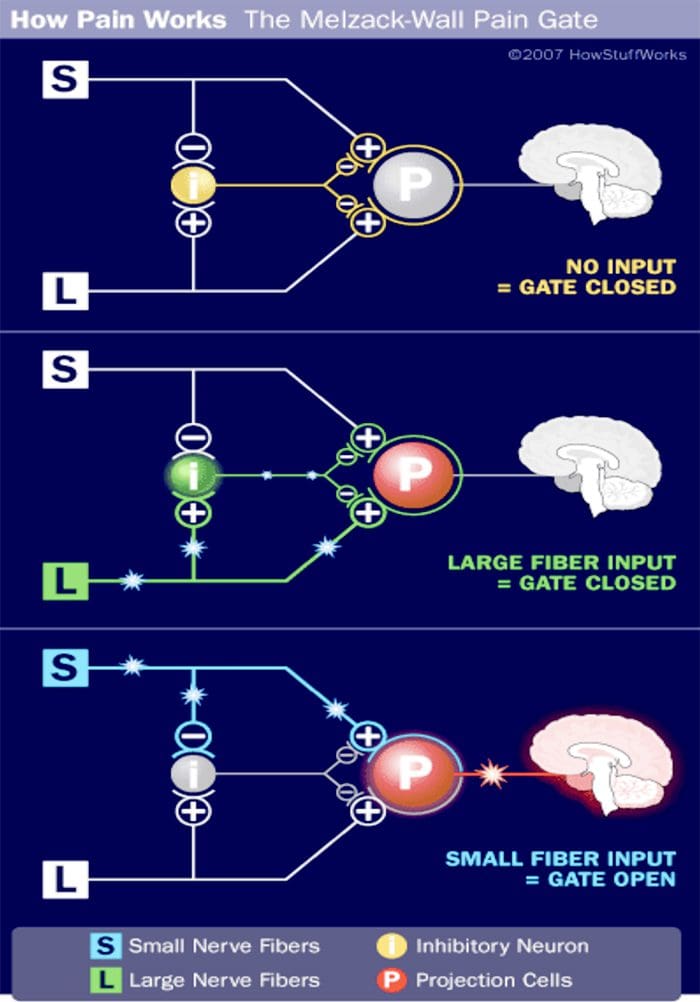
- This theory asserts non-nociceptive fibers can interfere with signals from pain fibers, therefore, inhibiting pain.
- Large-diameter A? fibers are nonnociceptive (do not transmit pain stimuli) and inhibit the effects of firing by A? and C fibers.
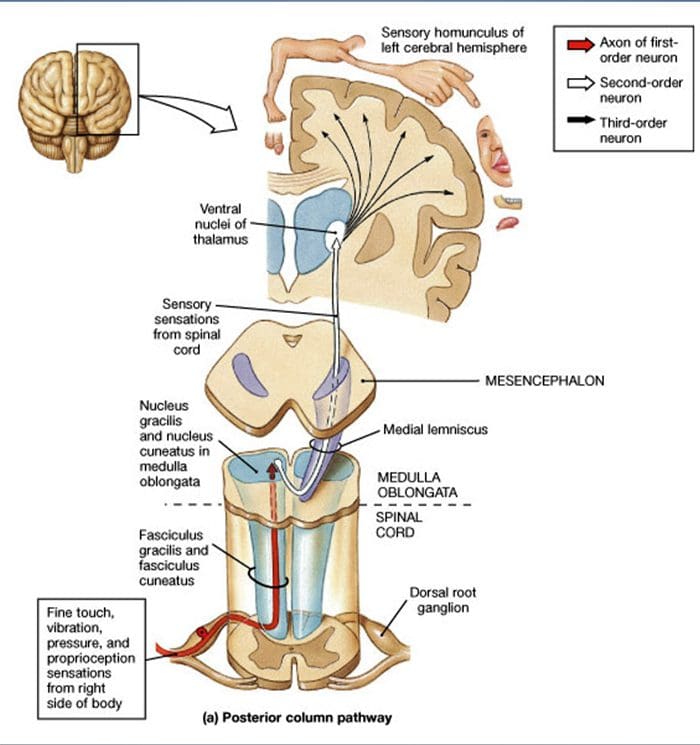
 DORSAL COLUMN MEDIAL LEMNISCAL PATHWAY
DORSAL COLUMN MEDIAL LEMNISCAL PATHWAY
 UTILIZATION OF PERIPHERAL MECHANORECEPTORS TO ALTER PAIN PERCEPTION
UTILIZATION OF PERIPHERAL MECHANORECEPTORS TO ALTER PAIN PERCEPTION
HOW CAN WE HELP?

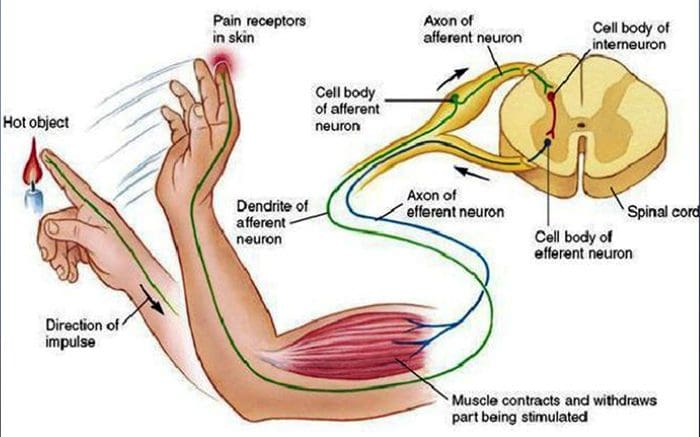
WITHDRAWAL REFLEX
- An excited afferent neuron stimulates excitatory interneurons that in turn stimulate the efferent motor neurons supplying the biceps, the muscle in the arm that flexes (bends) the elbow joint. Contraction of the biceps pulls the hand away from the hot stove.
- The afferent neuron also stimulates inhibitory interneurons that in turn inhibit the efferent neurons supplying the triceps to prevent it from contracting. This type of neuronal connection involving stimulation of the nerve supply to one muscle and simultaneous inhibition of the nerves to its antagonistic muscle is known as reciprocal inhibition.
- The afferent neuron still stimulates other interneurons that carry the signal up the spinal cord to the brain via an ascending pathway. Only when the impulse reaches the sensory area of the cortex is the person aware of the pain, its location and the type of stimulus. Moreover, when the impulse reaches the brain, the information can be stored as memory and the person can think about what happened.
RECEPTOR BASED THERAPY
Adjustments
- Activation of joint mechanoreceptors through chiropractic adjustments can modulate and “overshadow” the brains perception of smaller diameter fibers.
- Repetition of activation of joint mechanoreceptors can create positive plasticity in afferent pathways.
- Positive plasticity can shut down pain
Vibration
- Vibratory stimulation at specific frequencies can alter pain perception
- Repetition of activation of Merkel’s discs and Meissner’s corpuscles can create positive plasticity in afferent pathways.
- Again, positive plasticity can shut down pain
 VIBRATION
VIBRATION
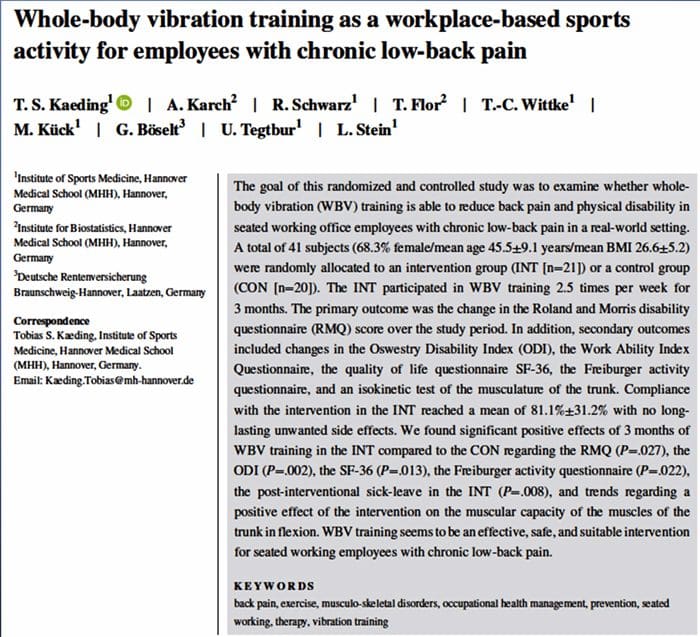
- “This type of device applies sinusoidal vibrations and offers continuous selectable amplitude of 0-5.2mm depending on the foot position and a selectable frequency of 5-30Hz.”
- “WBV training seems to be an effective, safe, and suitable intervention for seated working employees with chronic low-back pain.”
- “Homotopic vibro-tactile stimulation resulted in 40% heat pain reductions in all subject groups. Distraction did not seem to affect experimental pain ratings.”
- “Vibro-tactile stimulation effectively recruited analgesic mechanisms not only in NC but also in patients with chronic musculoskeletal pain, including FM.”
 LIGHT TOUCH
LIGHT TOUCH
- “In total, 44 healthy volunteers experienced heat pain and CT optimal (slow brushing) and CT sub-optimal (fast brushing or vibration) stimuli. Three different experimental paradigms were used: Concurrent application of heat pain and tactile (slow brushing or vibration) stimulation; Slow brushing, applied for variable duration and intervals, preceding heat pain; Slow versus fast brushing preceding heat pain.”
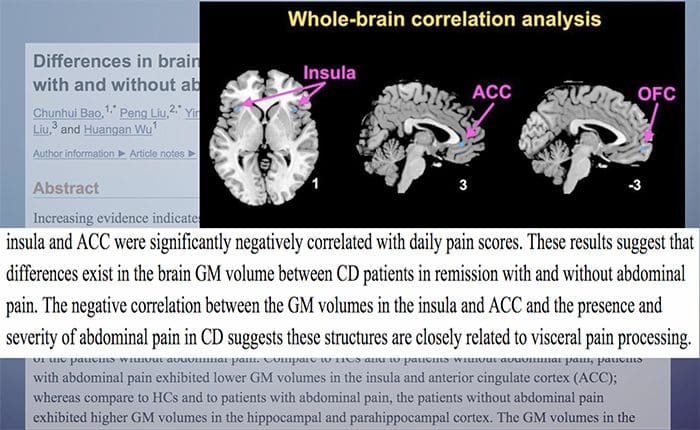
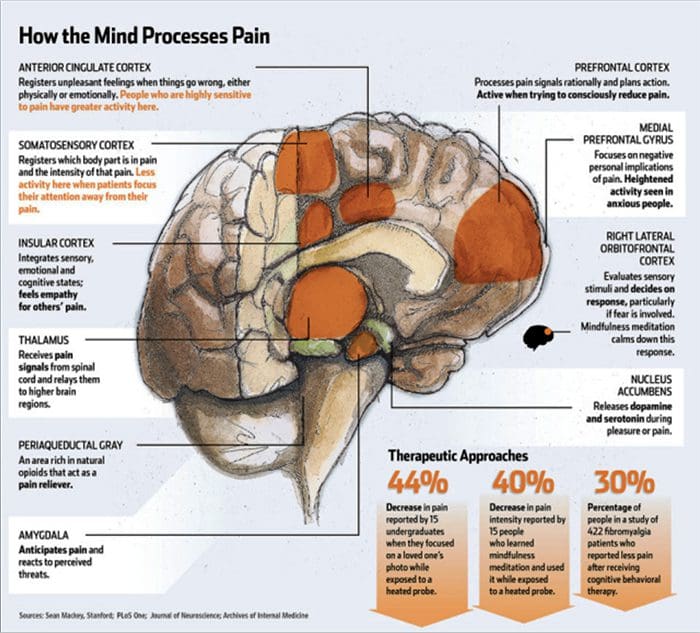
- In humans, the main brain areas receiving C- LTMR information belong to the somatosensory system and affect processing brain networks like the contralateral posterior insular cortex or the medial prefrontal cortex. The intensity of CT targeted touch is encoded in the primary and secondary somatosensory cortex (S1 contralateral, S2 bilateral), whereas the pleasantness is encoded in the anterior cingulate cortex. C-LTMRs also activate regions involved in reward processing (putamen and orbitofrontal cortex) and in processing of social stimuli (posterior superior temporal sulcus).

EVERYTHING PERIPHERAL HAS A CENTRAL CONSEQUENCE
 CASE STUDY
CASE STUDY
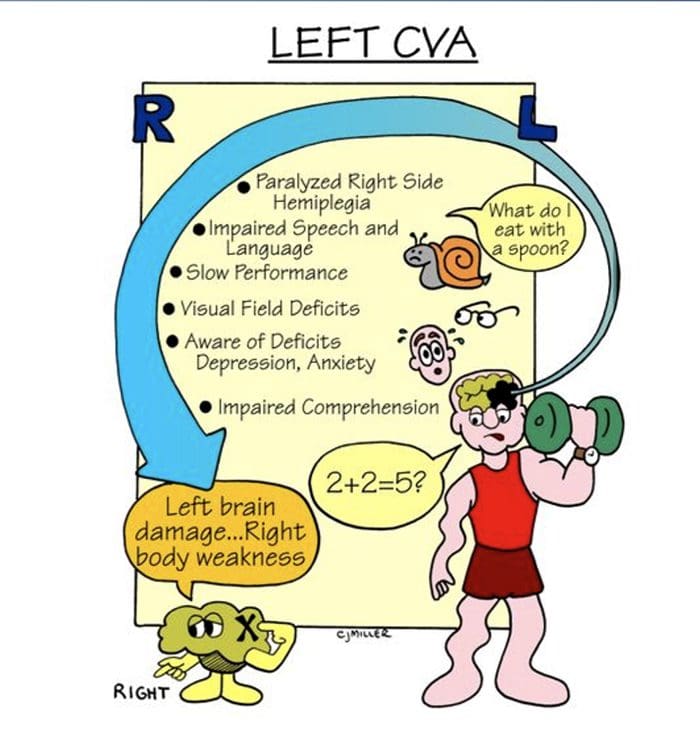
- 47-year-old male suffered left CVA in October of 2017.
- Has not moved the right side of his body since the accident.
- Presented to our clinic because he wants to ”get back to it.”
 PHYSICAL EXAMINATION HIGHLIGHTS
PHYSICAL EXAMINATION HIGHLIGHTS
- Dysarthria
- Altered pain perception
- Difficulty with simple math
- Flaccid on RUE and RLE
 PHYSICAL EXAMINATION HIGHLIGHTS
PHYSICAL EXAMINATION HIGHLIGHTS
- Patient had no movement until we began testing sensation and reflexes:

ALLODYNIA: Refers to central pain sensitization ( increased response of neurons) following normally non-painful, often repetitive stimulation.
- Allodynia can lead to the triggering of a pain response from stimuli, which does not normally provoke pain.
- Temperature or physical stimuli can provoke allodynia, which may feel like a burning sensation and it often occurs after injury to a site.
- Alldynia is different from Hyperalgesia, an extreme, exaggerated reaction to a stimulus, which is normally painful.
THERAPEUTIC INTERVENTIONS
- Vibration
- Light Touch
- Acupressure
- Acoustic Frequencies
- Adjustments!
 AFTER TWO DAYS
AFTER TWO DAYS


Mechanoreceptive Pain & Receptor Based Therapy
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card