


For individuals trying to retrain their body movements for back health improvement, what is the spinal area that helps the body twist, bend, and stand upright?
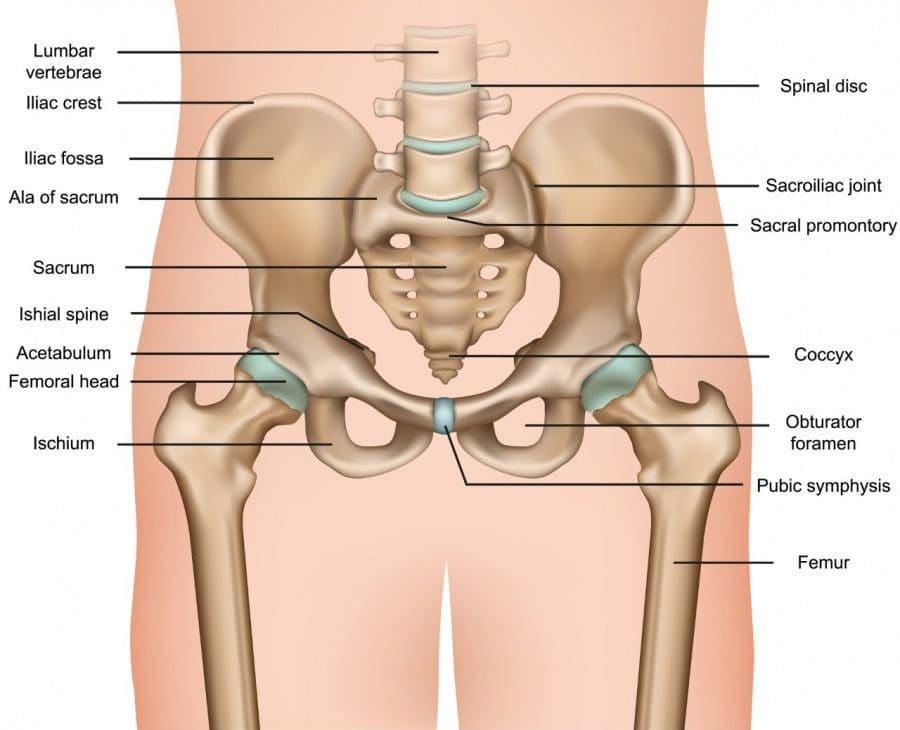
Table of Contents
Lumbosacral Joint L5-S1
The L5-S1, also called the lumbosacral joint, is a term used to describe a part of the spine. It is where the lumbar spine ends and the sacral spine begins, and it connects these bones. The lumbosacral joint is also susceptible to misalignment and injury, such as disc herniation or a spinal disorder called spondylolisthesis.
The spinal column is the structure that allows the body to stand upright and helps you twist, bend, and alter trunk and neck position. Typically, 24 movable bones in the spine connect to the sacrum and the coccyx, or the tailbone. The sacrum and the coccyx each have multiple bones that fuse over time. L5-S1 consists of the last bone in the lumbar spine, called L5, and the triangle-shaped bone under it, known as the sacrum. S1 is at the top of the sacrum and comprises five fused bones.
Risk of Injury
Each area of the spine has a curve that goes in opposite directions. The places where the spinal curve directions change are junctional levels. The risk of injuries may be higher at junctional levels because the body weight shifts direction as the curves shift. The L5-S1 junction is located between the lumbar curve and the sacral curve. The lumbar curve sweeps forward, and the sacral curve goes backward.
The lumbosacral joint L5-S1 junction is highly vulnerable to misalignment, wear and tear, and injury. This is because the top of the sacrum is positioned at an angle for most individuals. Aging and injury increase the vulnerability of the L5-S1 junction even more. Pain coming from L5-S1 is usually treated with:
- Heat and/or ice
- Over-the-counter anti-inflammatory medications
- Prescription pain medications
- Muscle relaxers
- Physical therapy
- Chiropractic adjustments
- Epidural steroid injections
If these therapies do not help, surgery may be recommended. L5-S1 is one of the two most common sites for back surgery.
Conditions
Disc herniation at L5-S1 is a common injury and cause of sciatica, which can cause pain and other issues (MedlinePlus, 2024). The L5-S1 junction is often the site of a condition known as spondylolisthesis.
Disc Herniation
Discs separate the vertebrae, cushioning the spinal column and allowing movement between vertebrae. A disc herniation means the disc slips out of place. (MedlinePlus, 2022) A disc herniation at L5-S1 is a common cause of sciatica. Symptoms of sciatica include:
- Burning
- Numbness
- Pain or tingling that radiates from the buttock down the leg to the knee or foot.
- The pain is often sharp and can feel like an electric shock. (American Association of Neurological Surgeons, 2024)
Disc herniation can also cause chronic back pain and stiffness and trigger painful muscle spasms. Bowel problems are also possible with disc issues at L5-S1. Research links irritable bowel syndrome to herniated discs in the lower back. (Bertilson BC, Heidermakr A, Stockhaus M. 2015) Additional studies found disc problems at L5-S1 can lead to difficulty with sphincter control. (Akca N. et al., 2014) Initial treatments for disc herniation include rest and pain relievers to reduce inflammation and swelling, then physical therapy. Most recover with conservative interventions, and those who don’t may require a steroid injection or surgery. (MedlinePlus, 2022)
Spondylolisthesis
Spondylolisthesis occurs when a vertebra slips forward relative to the bone below it. The most common form of this condition is degenerative spondylolisthesis, which generally begins when the spine wears down with age. Isthmic spondylolisthesis is another common variation and starts as a tiny fracture in the pars interarticularis, a bone that connects the adjoining parts of the facet joint. (American Academy of Orthopaedic Surgeons, 2020) These fractures often occur before age 15, but symptoms do not develop until adulthood. Degeneration of the spine in later adulthood can further worsen the condition.
The angle of the sacrum can also contribute to spondylolisthesis. This is because the S1 tips down in the front and up in the back rather than being horizontal. Individuals with a greater tilt are usually at a higher risk of spondylolisthesis. (Gong S. et al., 2019) However, individuals with spondylolisthesis may not have any symptoms. Those who do may experience: (American Academy of Orthopaedic Surgeons, 2020)
- Back stiffness
- Standing difficulties
- Walking difficulties
- Lower back pain
- Hamstring tightness
Spondylolisthesis is typically treated with non-surgical interventions that can include:
- Pain medications
- Heat and/or ice application
- Physical therapy
- Epidural steroid injections
Usually, non-surgical care is tried for at least six months. If pain and symptoms persist, surgery may be an option. Spinal fusion surgery can be effective but requires a long recovery time and can have additional risks.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Chiropractic Healing After Trauma
References
MedlinePlus. (2024). Sciatica. Retrieved from https://medlineplus.gov/sciatica.html
MedlinePlus. (2022). Herniated disk. Retrieved from https://medlineplus.gov/ency/article/000442.htm
American Association of Neurological Surgeons. (2024). Herniate disc. https://www.aans.org/patients/conditions-treatments/herniated-disc/
Bertilson, B. C., Heidermark, A., & Stockhaus, M. (2015). Irritable Bowel Syndrome–a Neurological Spine Problem. Journal of Advances in Medicine and Medical Research, 4(24), 4154–4168. https://doi.org/10.9734/BJMMR/2014/9746
Akca, N., Ozdemir, B., Kanat, A., Batcik, O. E., Yazar, U., & Zorba, O. U. (2014). Describing a new syndrome in L5-S1 disc herniation: Sexual and sphincter dysfunction without pain and muscle weakness. Journal of craniovertebral junction & spine, 5(4), 146–150. https://doi.org/10.4103/0974-8237.147076
American Academy of Orthopaedic Surgeons. (2020). Spondylolysis and spondylolisthesis. https://orthoinfo.aaos.org/en/diseases–conditions/spondylolysis-and-spondylolisthesis/
Gong, S., Hou, Q., Chu, Y., Huang, X., Yang, W., & Wang, Z. (2019). Anatomical factors and pathological parts of isthmic fissure and degenerative lumbar spondylolisthesis.
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card