

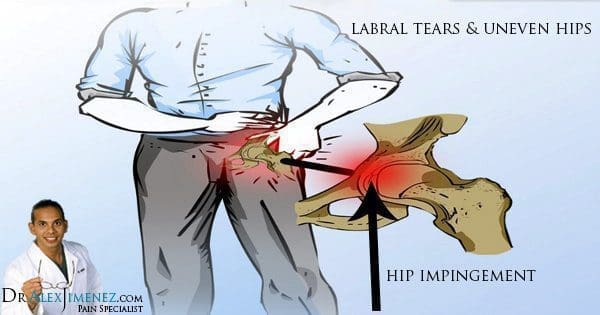
A majority of complications to the hip joint can often be related to acetabular labral tears, or ALT, and in up to 80 percent of cases, these can also be identified alongside intra-articular snapping hip syndrome. Labral tears in the joints of the hip account for hip and groin pain symptoms of approximately 22-55 percent of individuals affected by the injury. Research suggests that an untreated ALT may increase the risk of degenerative hip arthritis, which has created a widespread interest within many healthcare professionals.
In the past ten years, the examination and imaging techniques utilized to diagnose acetabular labral tears have been increasing greatly, although these assessments are still considered to be complex. Foremost, by reviewing the anatomy and biomechanics of the acetabular labrum, the evaluation techniques and the treatments, individuals can learn to understand the options for managing their labral tears.
Table of Contents
Anatomy of the Hip
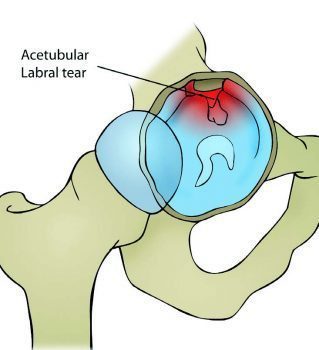
The labrum increases the surface area of the acetabulum by 22 percent while it increases the volume by 33 percent, functioning accordingly to fasten the head of the femur while allowing it to rotate. From a cross-sectional view, the labrum is triangular in shape with an extra articular area of thick connective tissue which contains a rich supply of blood while the intra articular area majorly has no blood supply.
When the hip’s normal range of mobility extends beyond its limit, the labrum is stressed by a strong, compressive force and a tear at his point can ultimately affect the stability of the joint and distribution of weight or load. Furthermore, the labrum is considered a pain generating structure as numerous pain receptors are located in its superior and anterior regions. It is at the anterior surface where an ALT is most vulnerable to pressure along the end point of hip flexion. On another note, abnormal alterations within the structure, such as retroverted acetabulum and coxa valga, have been simultaneously recorded in up to 87 percent of individuals with labral tears.
Evaluating Acetabular Labral Tears
Acetabular labral tears are difficult to diagnose and, despite of current advances in medical imaging and assessment techniques, one report established that on average, patients with an ALT visited three healthcare providers and waited for approximately 21 months before the injury was properly diagnosed. As a medical professional evaluates an individual with a suspected hip injury, femoro-acetabular impingement, or FAI, and acetabular cartilage damage as well as MRI imaging should be utilized to further support a diagnosis.
Acetabular labral tears are often caused by cutting, pivoting, twisting and repetitive movements from end range hip flexions frequently practiced among tennis players, football players and runners. Researchers from the New England Baptist hospital in Boston, USA identified 273 athletes who also had articular cartilage damage from the 436 labral tear arthroscopies analyzed, almost 62 percent. However, the exact nature of an ALT injury may not always be clear to the individual, as these may also be degenerative, congenital or traumatic in its occurrence.
During a physical assessment for any hip-related injuries, it is essential to be observant of other non-musculoskeletal related pathologies. Hip pain may be associated to acetabular labral tears but hip complications can also be the result of lumbar spine or pelvic girdle dysfunction, abdominal viscera and issues with the peripheral nervous system. Symptoms of pain while resting, pain at night, fever, night sweats, unexplained weight loss are indicators of a non-musculoskeletal pathology which may require referral for further examination by a specialized healthcare provider. Hip pain may also be related to the abdominal and pelvic organs and a musculoskeletal injury must not be presumed.
An individual with an undiagnosed ALT may also be affected with synovitis and experience joint inflammation which can force them to adopt positions of hip flexion, external rotation and slight abduction, causing the capsule to be at its largest potential volume to reduce the stress on the labrum. Positions which include flexion and or abduction have been determined to increase the overall weight on the labrum and these are consciously avoided.
The joined, compressing position of flexion, abduction and internal rotation, best referred to as FADDIR’s test, increases stress to the labrum but it is also a contributor to intra-articular hip pathology. Individuals with acetabular labral tears may also report pain while squatting, stepping up with the affected extremity, or while sitting in a chair with the hips positioned lower than the knees. Additionally, an individual with an ALT is unlikely to extend the hip fully when running as this places the greatest amount of weight to the anterior joint capsule, subsequently adding stress to the anterior labrum.
Surgical versus non-surgical treatment?
Hip arthroscopy is a popular treatment utilized for individuals presenting symptoms of an ALT longer than four weeks, which has also been confirmed by MRI, or magnetic resonance imaging, and/or MRA, or magnetic resonance arthrogram. Hip arthroscopy for an ALT may include either labral debridement or labral repair. Different from surgical repair, there is limited support for conservative treatments for acetabular labral tears. However, researchers from Sao Paulo, Brazil have provided a case series of four individuals that underwent a rehabilitation program for this type of hip injury without surgery. The four individuals were diagnosed by an MRI scan and underwent a 3-phase program with the first being pain control, hip stabilization, re-education and correction of abnormal joint movement. Phase two focused on restoring normal range of motion, muscular strength and started sensory motor training. The final phase of their rehabilitation program focused on preparing the athlete to return to their specific sport.
The four individuals involved in the case series were in their mid-twenties and were from both sedentary and athletic backgrounds. The outcome of the conservative rehabilitation program leads to the individual’s pain level decrease, improved function and corrected muscle imbalances. Their muscle strength increased with the hip flexors from 1 percent to 39 percent, hip abductors increased muscle strength from 18 percent to 56 percent and the hip extensors increased their muscle strength from 68 percent to 139 percent. The results of the research were considered limited, as the case series only evaluated four individuals but nevertheless, the outcome could provide a proper approach while a patient is awaiting an arthroscopy.
Rehabilitation
After undergoing surgery for an ALT, the evidence behind following through with rehabilitation is considered limited as well in terms of its evidence, both within the surgeons own rehabilitation protocols and the therapist’s expertise. Researchers from Tampa, USA, constructed a rehabilitation protocol for the patients to follow which the following protocol is largely based upon:
Phase 1 (weeks 1–4)
After experiencing an ALT, or acetabular labral tears, the individual should limit the amount of weight they place on their limb by 50 percent for approximately 7-10 days, with flexion limited to 90° for 14 days. A labral debridement, or the removal of damaged tissue or foreign objects from a wound, has no limits following a surgical procedure into abduction, internal or external rotation or extension. In contrast, repairing acetabular labral tears should maintain non-weight bearing or toe-touch weight bearing for three to six weeks after a surgical operation.
During labral repair, the individual should maintain conservative ranges of movement while internal and external rotation should be conservatively moved into for 3 weeks. It’s essential to remember that if other procedures are carried out, such as micro fracture repair, then protocols following a surgery may be different.
In the immediate time period following a surgical operation, it is essential to manage pain, reduce swelling and begin early carefully moving the affected limb, but it is also essential to focus on other factors such as core activation and abductor control. Decreased activity of the hip abductor muscles has been previously linked to various lower extremity injuries and symptoms, including anterior knee pain. Therefore, once the individual begins to restore the natural range of their hip, it is essential to encourage them to activate the deep hip and trunk stability muscles to prevent secondary injuries from developing in the future.
Phase 2 (weeks 5–7)
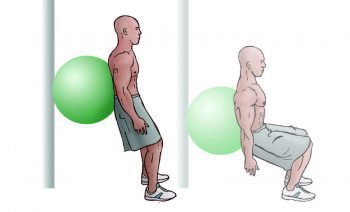
During this stage of rehabilitation, it is essential to restore normal range of movement while focusing on increasing strength and developing flexibility of the muscles crossing the hip joint.
Double Leg Standing Squats w/ Swiss Ball
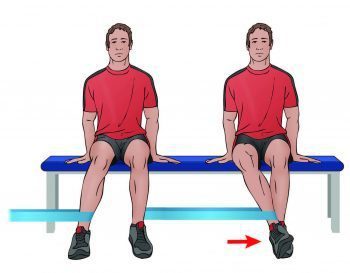
Seated Resistance: Internal/External Rotation
Double – Single Leg Bridging

Kneeling Hip Flexor Stretches

Side Stepping w/ Band Around Knees
Phase 3 (weeks 8-12)
While in this phase, the individual has a great opportunity to develop cardiovascular fitness and functional control of their hip. Functional stability exercises should be practiced in a standing position, making sure to maintain and improve stability in order for the individual to be able to return to their normal sport participation. Exercises to include in this phase are walking lunges, lunges with trunk rotation over the front leg and a Swiss ball program appropriate for challenging the core muscles.
Phase 4 (weeks 12+)
This phase of the rehabilitation program includes preparing the athlete for their return to their specific sport, emphasizing on specific protocols to train the individual around the task they will be performing. If the athlete is a defender in football, they should be replicating tasks specific to their position. Prior to the individual resuming full training, they must be able to demonstrate the same neuromuscular control as the unaffected side.
 In conclusion, an individual with suspected acetabular labral tears should have their injury confirmed using an MRI or MRA to properly determine the presence of an ALT but also to exclude any referred pain which could be signaling the presence of another musculoskeletal injury. An appropriate rehabilitation program should be started immediately to improve the function of the hip, control and to manage pain and ultimately restore the individual’s overall health. This will allow the athlete to proceed through any procedures with greater ease having already commenced a rehabilitation program.
In conclusion, an individual with suspected acetabular labral tears should have their injury confirmed using an MRI or MRA to properly determine the presence of an ALT but also to exclude any referred pain which could be signaling the presence of another musculoskeletal injury. An appropriate rehabilitation program should be started immediately to improve the function of the hip, control and to manage pain and ultimately restore the individual’s overall health. This will allow the athlete to proceed through any procedures with greater ease having already commenced a rehabilitation program.
For more information, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Chiropractic and Athletic Performance
Sourced through Scoop.it from: www.elpasochiropractorblog.com
By Dr. Alex Jimenez

TRENDING TOPIC: EXTRA EXTRA: New PUSH 24/7®? Fitness Center
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card