


Based on statistical findings, approximately more than three million people in the United States are injured in an automobile accident every year. In fact, auto accidents are considered to be one of the most common causes for trauma or injury. Neck injuries, such as whiplash, frequently occur due to the sudden back-and-forth movement of the head and neck from the force of the impact. The same mechanism of injury can also cause soft tissue injuries in other parts of the body, including the lower back as well as the lower extremities. Neck, hip, thigh and knee injuries are common types of injuries resulting from auto accidents.
Table of Contents
Abstract
- Objective: The purpose of this systematic review was to determine the effectiveness of exercise for the management of soft tissue injuries of the hip, thigh, and knee.
- Methods: We conducted a systematic review and searched MEDLINE, EMBASE, PsycINFO, the Cochrane Central Register of Controlled Trials, and CINAHL Plus with Full Text from January 1, 1990, to April 8, 2015, for randomized controlled trials (RCTs), cohort studies, and case-control studies evaluating the effect of exercise on pain intensity, self-rated recovery, functional recovery, health-related quality of life, psychological outcomes, and adverse events. Random pairs of independent reviewers screened titles and abstracts and assessed risk of bias using the Scottish Intercollegiate Guidelines Network criteria. Best evidence synthesis methodology was used.
- Results: We screened 9494 citations. Eight RCTs were critically appraised, and 3 had low risk of bias and were included in our synthesis. One RCT found statistically significant improvements in pain and function favoring clinicbased progressive combined exercises over a “wait and see” approach for patellofemoral pain syndrome. A second RCT suggests that supervised closed kinetic chain exercises may lead to greater symptom improvement than open chain exercises for patellofemoral pain syndrome. One RCT suggests that clinic-based group exercises may be more effective than multimodal physiotherapy in male athletes with persistent groin pain.
- Conclusion: We found limited high-quality evidence to support the use of exercise for the management of soft tissue injuries of the lower extremity. The evidence suggests that clinic-based exercise programs may benefit patients with patellofemoral pain syndrome and persistent groin pain. Further high-quality research is needed. (J Manipulative Physiol Ther 2016;39:110-120.e1)
- Key Indexing Terms: Knee; Knee Injuries; Hip; Hip Injuries; Thigh; Thigh Pain; Exercise
Soft tissue injuries of the lower limb are common. In the United States, 36% of all injuries presenting to emergency departments are sprains and/or strains of the lower extremity. Among Ontario workers, approximately 19% of all approved lost time compensation claims are related to lower extremity injuries. Moreover, 27.5% of Saskatchewan adults injured in a traffic collision report pain in the lower extremity. Soft tissue injuries of the hip, thigh, and knee are costly and place a significant economic and disability burden on workplaces and compensation systems. According to the US Department of Labor Bureau of Statistics, the median time off work for lower extremity injuries was 12 days in 2013. Knee injuries were associated with the longest work absenteeism (median, 16 days).
Most soft tissue injuries of the lower limb are managed conservatively, and exercise is commonly used to treat these injuries. Exercise aims to promote good physical health and restore normal function of the joints and surrounding soft tissues through concepts which include range of motion, stretching, strengthening, endurance, agility, and proprioceptive exercises. However, the evidence about the effectiveness of exercise for managing soft tissue injuries of the lower limb is unclear.
Previous systematic reviews have investigated the effectiveness of exercise for the management of soft tissue injuries of the lower extremity. Reviews suggest that exercise is effective for the management of patellofemoral pain syndrome and groin injuries but not for patellar tendinopathy. To our knowledge, the only review reporting on the effectiveness of exercise for acute hamstring injuries found little evidence to support stretching, agility, and trunk stability exercises.

The purpose of our systematic review was to investigate the effectiveness of exercise compared to other interventions, placebo/sham interventions, or no intervention in improving self-rated recovery, functional recovery (eg, return to activities, work, or school), or clinical outcomes (eg, pain, health-related quality of life, depression) of patients with soft tissue injuries of the hip, thigh, and knee.
Methods
Registration
This systematic review protocol was registered with the International Prospective Register of Systematic Reviews on March 28, 2014 (CRD42014009140).
Eligibility Criteria
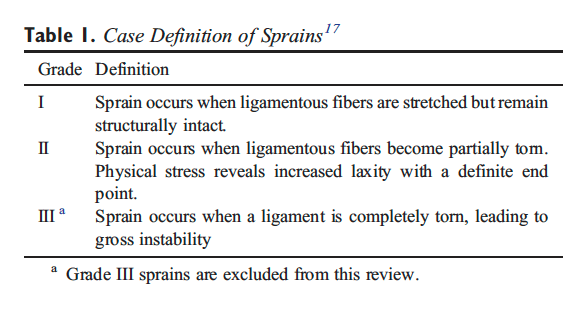
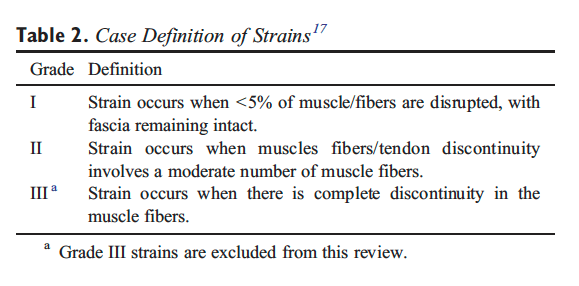
Population. Our review targeted studies of adults (?18 years) and/or children with soft tissue injuries of the hip, thigh, or knee. Soft tissue injuries include but are not limited to grade I to II sprains/strains; tendonitis; tendinopathy; tendinosis; patellofemoral pain (syndrome); iliotibial band syndrome; nonspecific hip, thigh, or knee pain (excluding major pathology); and other soft tissue injuries as informed by available evidence. We defined the grades of sprains and strains according to the classification proposed by the American Academy of Orthopaedic Surgeons (Tables 1 and 2). Affected soft tissues in the hip include the supporting ligaments and muscles crossing the hip joint into the thigh (including the hamstrings, quadriceps, and adductor muscle groups). Soft tissues of the knee include the supporting intra-articular and extra-articular ligaments and muscles crossing the knee joint from the thigh including the patellar tendon. We excluded studies of grade III sprains or strains, acetabular labral tears, meniscal tears, osteoarthritis, fractures, dislocations, and systemic diseases (eg, infection, neoplasm, inflammatory disorders).
Interventions. We restricted our review to studies that tested the isolated effect of exercise (ie, not part of a multimodal program of care). We defined exercise as any series of movements aimed at training or developing the body by routine practice or as physical training to promote good physical health.
Comparison Groups. We included studies that compared 1 or more exercise interventions to one another or one exercise intervention to other interventions, wait list, placebo/sham interventions, or no intervention.
Outcomes. To be eligible, studies had to include one of the following outcomes: (1) self-rated recovery; (2) functional recovery (eg, disability, return to activities, work, school, or sport); (3) pain intensity; (4) health-related quality of life; (5) psychological outcomes such as depression or fear; and (6) adverse events.
Study Characteristics. Eligible studies met the following criteria: (1) English language; (2) studies published between January 1, 1990, and April 8, 2015; (3) randomized controlled trials (RCTs), cohort studies, or case-control studies which are designed to assess the effectiveness and safety of interventions; and (4) included an inception cohort of a minimum of 30 participants per treatment arm with the specified condition for RCTs or 100 participants per group with the specified condition in cohort studies or case-control studies. Studies including other grades of sprains or strains in the hip, thigh, or knee had to provide separate results for participants with grades I or II sprains/strains to be included.
We excluded studies with the following characteristics: (1) letters, editorials, commentaries, unpublished manuscripts, dissertations, government reports, books and book chapters, conference proceedings, meeting abstracts, lectures and addresses, consensus development statements, or guideline statements; (2) study designs including pilot studies, cross-sectional studies, case reports, case series, qualitative studies, narrative reviews, systematic reviews (with or without meta-analyses), clinical practice guidelines, biomechanical studies, laboratory studies, and studies not reporting on methodology; (3) cadaveric or animal studies; and (4) studies on patients with severe injuries (eg, grade III sprains/strains, fractures, dislocations, full ruptures, infections, malignancy, osteoarthritis, and systemic disease).
Information Sources
We developed our search strategy with a health sciences librarian (Appendix 1). The Peer Review of Electronic Search Strategies (PRESS) Checklist was used by a second librarian to review the search strategy for completeness and accuracy. We searched MEDLINE and EMBASE, considered to be the major biomedical databases, and PsycINFO, for psychological literature through Ovid Technologies, Inc; CINAHL Plus with Full Text for nursing and allied health literature through EBSCOhost; and the Cochrane Central Register of Controlled Trials through Ovid Technologies, Inc, for any studies not captured by the other databases. The search strategy was first developed in MEDLINE and subsequently adapted to the other bibliographic databases. Our search strategies combined controlled vocabulary relevant to each database (eg, MeSH for MEDLINE) and text words relevant to exercise and soft tissue injuries of the hip, thigh, or knee including grade I to II sprain or strain injuries (Appendix 1). We also hand searched the reference lists of previous systematic reviews for any additional relevant studies.
Study Selection
A 2-phase screening process was used to select eligible studies. Random pairs of independent reviewers screened citation titles and abstracts to determine the eligibility of studies in phase 1. Screening resulted in studies being classified as relevant, possibly relevant, or irrelevant. In phase 2, the same pairs of reviewers independently screened the possibly relevant studies to determine eligibility. Reviewers met to reach consensus on the eligibility of studies and resolve disagreements. A third reviewer was used if consensus could not be reached.

Assessment of Risk of Bias
Independent reviewers were randomly paired to critically appraise the internal validity of eligible studies using the Scottish Intercollegiate Guidelines Network (SIGN) criteria. The impact of selection bias, information bias, and confounding on the results of a study was qualitatively evaluated using the SIGN criteria. These criteria were used to guide reviewers in making an informed overall judgment on the internal validity of studies. This methodology has been previously described. A quantitative score or a cutoff point to determine the internal validity of studies was not used for this review.
The SIGN criteria for RCTs were used to critically appraise the following methodological aspects: (1) clarity of the research question, (2) randomization method, (3) concealment of treatment allocation, (4) blinding of treatment and outcomes, (5) similarity of baseline characteristics between/among treatment arms, (6) cointervention contamination, (7) validity and reliability of outcome measures, (8) follow-up rates, (9) analysis according to intention-to-treat principles, and (10) comparability of results across study sites (where applicable). Consensus was reached through reviewer discussion. Disagreements were resolved by an independent third reviewer when consensus could not be reached. The risk of bias of each appraised study was also reviewed by a senior epidemiologist (PC). Authors were contacted when additional information was needed to complete the critical appraisal. Only studies with low risk of bias were included in our evidence synthesis.
Data Extraction and Synthesis of Results
Data were extracted from studies (DS) with low risk of bias to create evidence tables. A second reviewer independently checked the extracted data. We stratified results based on the duration of the condition (recent onset [0-3 months], persistent [N3 months], or variable duration [recent onset and persistent combined]).
We used standardized measures to determine the clinical importance of changes reported in each trial for common outcome measures. These include a between-group difference of 2/10 points on the Numeric Rating Scale (NRS), 2/10 cm difference on the Visual Analog Scale (VAS), and 10/100 point difference on the Kujala Patellofemoral scale, otherwise known as the Anterior Knee Pain Scale.
Statistical Analyses
Agreement between reviewers for the screening of articles was computed and reported using the ? statistic and 95% confidence interval (CI). Where available, we used data provided in the studies with a low risk of bias to measure the association between the tested interventions and the outcomes by computing the relative risk (RR) and its 95% CI. Similarly, we computed differences in mean changes between groups and 95% CI to quantify the effectiveness of interventions. The calculation of 95% CIs was based on the assumption that baseline and follow-up outcomes were highly correlated (r = 0.80).
Reporting
This systematic review was organized and reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.
Dr. Alex Jimenez’s Insight
As a doctor of chiropractic, automobile accident injuries are one of the most common reasons people seek chiropractic care. From neck injuries, such as whiplash, to headaches and back pain, chiropractic can be utilized to safely and effectively restore the integrity of the spine after a car crash. A chiropractor like myself will often use a combination of spinal adjustments and manual manipulations, as well as a variety of other non-invasive treatment methods, to gently correct any spinal misalignments resulting from an auto accident injury. Whiplash and other types of neck injuries occur when the complex structures along the cervical spine are stretched beyond their natural range of movement due to the sudden back-and-forth movement of the head and neck from the force of the impact. Back injury, particularly in the lower spine, are also common as a result of an automobile accident. When the complex structures along the lumbar spine are damaged or injured, symptoms of sciatica may radiate down the lower back, into the buttocks, hips, thighs, legs and down into the feet. Knee injuries may also occur upon impact during an auto accident. Exercise is frequently used with chiropractic care to help promote recovery as well as improve strength, flexibility and mobility. Rehabilitation exercises are offered to patients to further restore the integrity of their body. The following research studies demonstrate that exercise, compared to non-invasive treatment options, is a safe and effective treatment method for individuals suffering with neck and lower extremity injury from a car crash.
Results
Study Selection
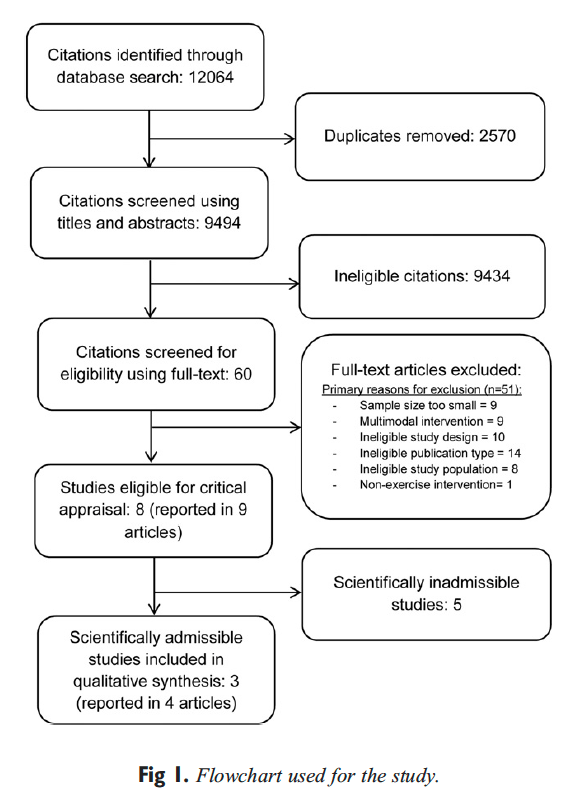
We screened 9494 citations based on the title and abstract (Figure 1). Of these, 60 full-text publications were screened, and 9 articles were critically appraised. The primary reasons for ineligibility during full text screening were (1) ineligible study design, (2) small sample size (n b 30 per treatment arm), (3) multimodal interventions not allowing isolation of the effectiveness of exercise, (4) ineligible study population, and (5) interventions not meeting our definition of exercise (Figure 1). Of those critically appraised, 3 studies (reported in 4 articles) had low risk of bias and were included in our synthesis. The interrater agreement for the screening of the articles was ? = 0.82 (95% CI, 0.69-0.95). The percentage agreement for the critical appraisal of studies was 75% (6/8 studies). Disagreement was resolved through discussion for 2 studies. We contacted authors from 5 studies during critical appraisal to request additional information and 3 responded.
Study Characteristics
The studies with low risk of bias were RCTs. One study, conducted in the Netherlands, examined the effectiveness of a standardized exercise program compared to a “wait and see” approach in participants with patellofemoral pain syndrome of variable duration. A second study, with outcomes reported in 2 articles, compared the benefit of closed vs open kinetic chain exercises in individuals with variable duration patellofemoral pain syndrome in Belgium. The final study, conducted in Denmark, investigated active training compared to a multimodal physiotherapy intervention for the management of persistent adductor-related groin pain.
Two RCTs used exercise programs that combined strengthening exercises with balance or agility training for the lower extremity. Specifically, the strengthening exercises consisted of both isometric and concentric contractions of the quadriceps, hip adductor, and gluteal muscles for the management of patellofemoral pain46 and hip adductors and muscles of the trunk and pelvis for adductor-related groin pain. The exercise programs ranged from 646 to 1243 weeks in duration and were supervised and clinic based with additional daily home exercises. The exercise programs were compared to a “wait and see” approach or to multimodal physiotherapy. The third RCT compared 2 different 5-week protocols which combined either closed or open kinetic chain strengthening and stretching exercises for the lower extremity musculature.
Meta-analysis was not performed due to heterogeneity of accepted studies with respect to patient populations, interventions, comparators, and outcomes. Principles of best evidence synthesis were used to develop evidence statements and perform a qualitative synthesis of findings from studies with low risk of bias.
Risk of Bias Within Studies
The studies with low risk of bias had a clearly defined research question, used appropriate blinding methods where possible, reported adequate similarity of baseline characteristics between treatment arms, and performed an intention-to-treat analyses where applicable (Table 3). The RCTs had follow-up rates greater than 85%. However, these studies also had methodological limitations: insufficient detail describing methods for allocation concealment (1/3), insufficient detail describing methods of randomization (1/3), the use of outcome measures that have not been demonstrated to be valid or reliable (ie, muscle length and successful treatment) (2/3), and clinically important differences in baseline characteristics (1/3).
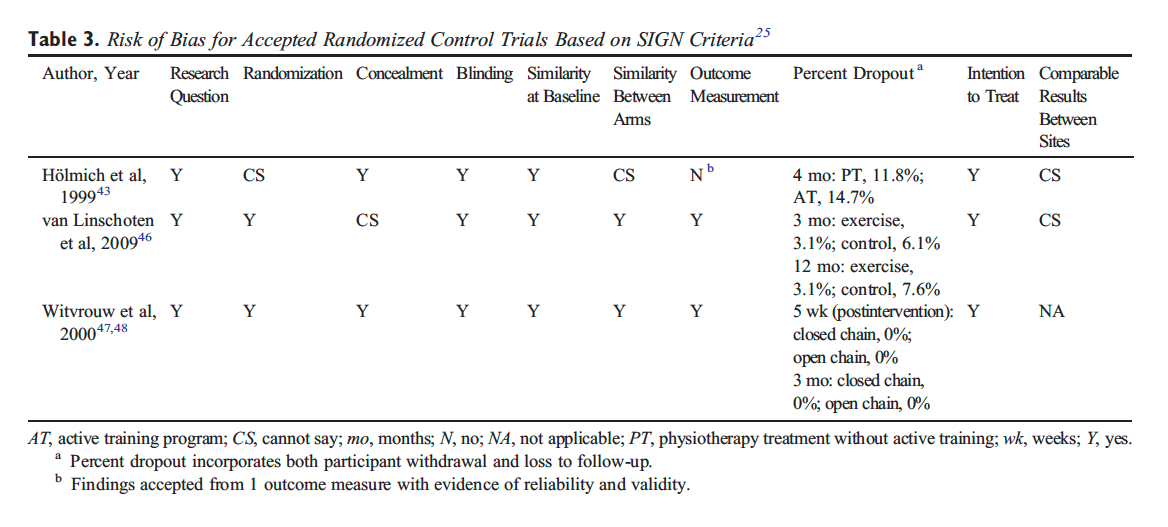
Of 9 relevant articles, 5 were deemed to have high risk of bias. These studies had the following limitations: (1) poor or unknown randomization methods (3/5); (2) poor or unknown allocation concealment methods (5/ 5); (3) outcome assessor not blinded (4/ 5); (4) clinically important differences in baseline characteristics (3/5); (5) dropouts not reported, insufficient information regarding dropouts per group or large differences in dropout rates between treatment arms (N15%) (3/5); and (6) a lack of information about or no intention-to-treat analysis (5/5).
Summary of Evidence
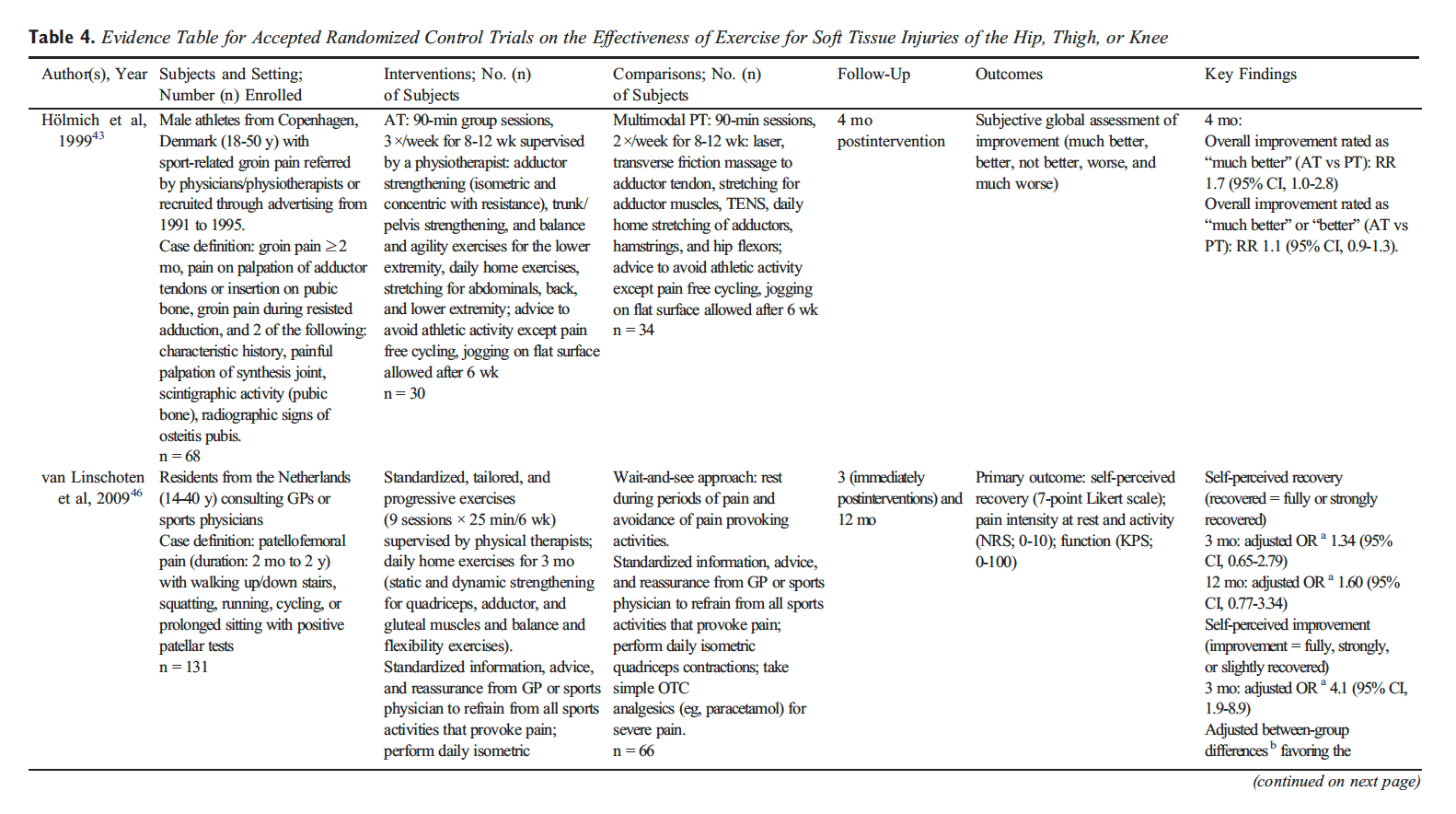
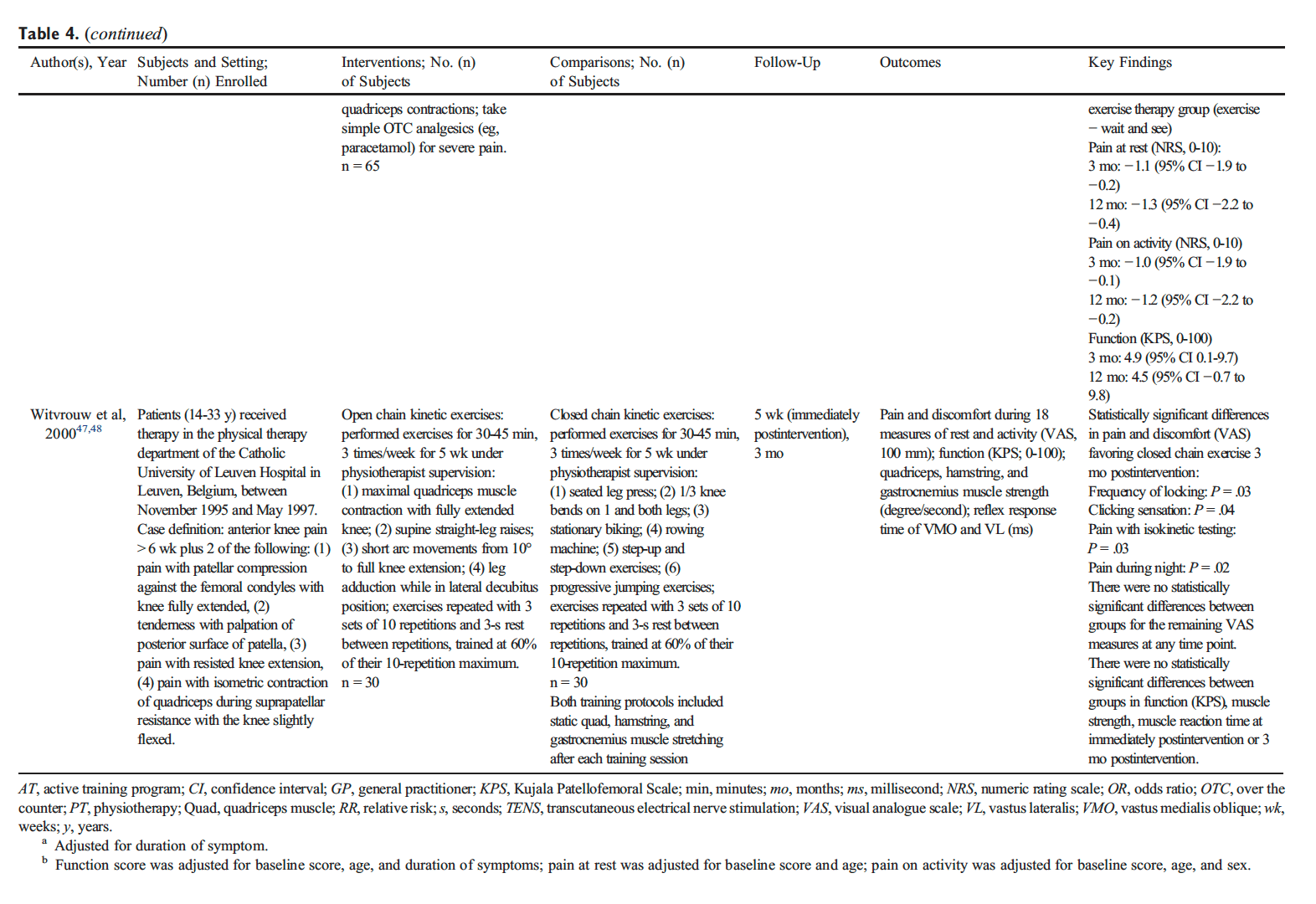
Patellofemoral Pain Syndrome of Variable Duration. Evidence from 1 RCT suggests that a clinic-based progressive exercise program may provide short- and long-term benefit over usual care for the management of patellofemoral pain syndrome of variable duration. van Linschoten et al randomized participants with a clinical diagnosis of patellofemoral pain syndrome of 2 months to 2 years duration to (1) a clinic-based exercise program (9 visits over 6 weeks) consisting of progressive, static, and dynamic strengthening exercises for the quadriceps, adductor, and gluteal muscles and balance and flexibility exercises, or (2) a usual care “wait and see” approach. Both groups received standardized information, advice, and home-based isometric exercises for the quadriceps based on recommendations from Dutch General Practitioner guidelines (Table 4). There were statistically significant differences favoring the exercise group for (1) pain (NRS) at rest at 3 months (mean change difference 1.1/10 [95% CI, 0.2-1.9]) and 6 months (mean change difference 1.3/10 [95% CI, 0.4-2.2]); (2) pain (NRS) with activity at 3 months (mean change difference 1.0/10 [95% CI, 0.1-1.9]) and 6 months (mean change difference 1.2/10 [95% CI, 0.2-2.2]); and (3) function (Kujala Patellofemoral Scale [KPS]) at 3 months (mean change difference 4.9/100 [95% CI, 0.1-9.7]). However, none of these differences were clinically important. Furthermore, there were no significant differences in the proportion of participants reporting recovery (fully recovered, strongly recovered), but the exercise group was more likely to report improvement at 3-month follow-up (odds ratio [OR], 4.1 [95% CI, 1.9-8.9]).

Evidence from a second RCT suggests that physiotherapist- supervised closed kinetic chain leg exercises (where the foot remains in constant contact with a surface) may provide short-term benefit compared to supervised open kinetic chain exercises (where the limb moves freely) for some patellofemoral pain syndrome symptoms (Table 4). All participants trained for 30 to 45 minutes, 3 times per week for 5 weeks. Both groups were instructed to perform static lower limb stretching after each training session. Those randomized to closed chain exercises performed supervised (1) leg presses, (2) knee bends, (3) stationary biking, (4) rowing, (5) step-up and step-down exercises, and (6) progressive jumping exercises. Open chain exercise participants performed (1) maximal quad muscle contraction, (2) straight-leg raises, (3) short arc movements from 10° to full knee extension, and (4) leg adduction. Effect sizes were not reported, but the authors reported statistically significant differences favoring closed kinetic chain exercise at 3 months for (1) frequency of locking (P = .03), (2) clicking sensation (P = .04), (3) pain with isokinetic testing (P = .03), and (4) pain during night (P = .02). The clinical significance of these results is unknown. There were no statistically significant differences between groups for any other pain or functional measures at any follow-up period.
Persistent Adductor-Related Groin Pain
Evidence from 1 RCT suggests that a clinic-based group exercise program is more effective than a multimodal program of care for persistent adductor-related groin pain. Hölmich et al studied a group of male athletes with a clinical diagnosis of adductor-related groin pain of greater than 2 months duration (median duration, 38-41 weeks; range, 14-572 weeks) with or without osteitis pubis. Participants were randomized to (1) a clinic-based group exercise program (3 sessions per week for 8-12 weeks) consisting of isometric and concentric resistance strengthening exercises for the adductors, trunk, and pelvis; balance and agility exercises for the lower extremity; and stretching for the abdominals, back, and lower extremity (with the exception of the adductor muscles) or (2) a multimodal physiotherapy program (2 visits per week for 8-12 weeks) consisting of laser; transverse friction massage; transcutaneous electrical nerve stimulation (TENS); and stretching for the adductors, hamstrings, and hip flexors (Table 4). Four months after the intervention, the exercise group was more likely to report that their condition was “much better” (RR, 1.7 [95% CI, 1.0-2.8]).
Adverse Events
None of the included studies commented on the frequency or nature of adverse events.
Discussion
Summary of Evidence
Our systematic review examined the effectiveness of exercise for the management of soft tissue injuries of the hip, thigh, or knee. Evidence from 1 RCT suggests that a clinic-based progressive combined exercise program may offer additional short- or long-term benefit compared to providing information and advice for the management of patellofemoral pain syndrome of variable duration. There is also evidence that supervised closed kinetic chain exercises may be beneficial for some patellofemoral pain syndrome symptoms compared to open kinetic chain exercises. For persistent adductor-related groin pain, evidence from 1 RCT suggests that a clinic-based group exercise program is more effective than a multimodal program of care. Despite the common and frequent use of exercise prescription, there is limited high-quality evidence to inform the use of exercise for the management of soft tissue injuries of the lower extremity. Specifically, we did not find high-quality studies on exercise for the management of some of the more commonly diagnosed conditions including patellar tendinopathy, hamstring sprain and strain injuries, hamstring tendinopathy, trochanteric bursitis, or capsular injuries of the hip.

Previous Systematic Reviews
Our results are consistent with findings from previous systematic reviews, concluding that exercise is effective for the management of patellofemoral pain syndrome and groin pain. However, the results from previous systematic reviews examining the use of exercise for the management of patellar tendinopathy and acute hamstring injuries are inconclusive. One review noted strong evidence for use of eccentric training, whereas others reported uncertainty of whether isolated eccentric exercises were beneficial for tendinopathy compared to other forms of exercise. Furthermore, there is limited evidence of a positive effect from stretching, agility and trunk stability exercises, or slump stretching for the management of acute hamstring injuries. Differing conclusions between systematic reviews and the limited number of studies deemed admissible in our work may be attributed to differences in methodology. We screened reference lists of previous systematic reviews, and most studies included in the reviews did not meet our inclusion criteria. Many studies accepted in other reviews had small sample sizes (b30 per treatment arm). This increases the risk of residual confounding while also reducing the effect size precision. Furthermore, a number of systematic reviews included case series and case studies. These types of studies are not designed to assess the effectiveness of interventions. Finally, previous reviews included studies where exercise was part of a multimodal intervention, and as a consequence, the isolated effect of exercise could not be ascertained. Of the studies that satisfied our selection criteria, all were critically appraised in our review, and only 3 had low risk of bias and were included in our synthesis.
Strengths
Our review has many strengths. First, we developed a rigorous search strategy that was independently reviewed by a second librarian. Second, we defined clear inclusion and exclusion criteria for the selection of possibly relevant studies and only considered studies with adequate sample sizes. Third, pairs of trained reviewers screened and critically appraised eligible studies. Fourth, we used a valid set of criteria (SIGN) to critically appraise studies. Finally, we restricted our synthesis to studies with low risk of bias.
Limitations and Recommendations for Future Research
Our review also has limitations. First, our search was limited to studies published in the English language. However, previous reviews have found that the restriction of systematic reviews to English language studies has not led to a bias in reported results. Second, despite our broad definition of soft tissue injuries of the hip, thigh, or knee, our search strategy may not have captured all potentially relevant studies. Third, our review may have missed potentially relevant studies published before 1990. We aimed to minimize this by hand searching the reference lists of previous systematic reviews. Finally, critical appraisal requires scientific judgment that may differ between reviewers. We minimized this potential bias by training reviewers in the use of the SIGN tool and using a consensus process to determine study admissibility. Overall, our systematic review highlights a deficit of strong research in this area.
High-quality studies on the effectiveness of exercise for the management of soft tissue injuries of the lower extremity are needed. Most studies included in our review (63%) had a high risk of bias and could not be included in our synthesis. Our review identified important gaps in the literature. Specifically, studies are needed to inform the specific effects of exercises, their long-term effects, and the optimal doses of intervention. Furthermore, studies are needed to determine the relative effectiveness of different types of exercise programs and if the effectiveness varies for soft tissue injuries of the hip, thigh, and knee.
Conclusion
There is limited high-quality evidence to inform the use of exercise for the management of soft tissue injuries of the hip, thigh, and knee. The current evidence suggests that a clinic-based progressive combined exercise program may lead to improved recovery when added to information and advice on resting and avoiding pain provoking activities for the management of patellofemoral pain syndrome. For persistent adductor-related groin pain, a supervised clinic- based group exercise program is more effective than multimodal care in promoting recovery.
Funding Sources and Potential Conflicts of Interest
This study was funded by the Ontario Ministry of Finance and the Financial Services Commission of Ontario (RFP no. OSS_00267175). The funding agency was not involved in the collection of data, data analysis, interpretation of data, or drafting of the manuscript. The research was undertaken, in part, thanks to funding from the Canada Research Chairs program. Pierre Côté has previously received funding from a Grant from the Ontario Ministry of Finance; consulting for the Canadian Chiropractic Protective Association; speaking and/or teaching arrangements for the National Judicial Institute and Société des Médecins Experts du Quebec; trips/travel, European Spine Society; board of directors, European Spine Society; grants: Aviva Canada; fellowship support, Canada Research Chair Program–Canadian Institutes of Health Research. No other conflicts of interest were reported for this study.
Contributorship Information
- Concept development (provided idea for the research): D.S., C.B., P.C., J.W., H.Y., S.V.
- Design (planned the methods to generate the results): D.S., C.B., P.C., H.S., J.W., H.Y., S.V.
- Supervision (provided oversight, responsible for organization and implementation, writing of the manuscript): D.S., P.C.
- Data collection/processing (responsible for experiments, patient management, organization, or reporting data): D.S., C.B., H.S., J.W., D.e.S., R.G., H.Y., K.R., J.C., K.D., P.C., P.S., R.M., S.D., S.V.
- Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): D.S., C.B., P.C., H.S., M.S., K.R., L.C.
- Literature search (performed the literature search): A.T.V.
- Writing (responsible for writing a substantive part of the manuscript): D.S., C.B., P.C., H.S.
- Critical review (revised manuscript for intellectual content, this does not relate to spelling and grammar checking): D.S., P.C., H.S., J.W., D.e.S., R.G., M.S., A.T.V., H.Y., K.R., J.C., K.D., L.C., P.S., S.D., R.M., S.V.
Practical Applications
- There is evidence to suggest that clinic-based exercises may benefit patients with patellofemoral pain syndrome or adductor-related groin pain.
- Supervised progressive exercises may be beneficial for patellofemoral pain syndrome of variable duration compared to information/advice.
- Supervised closed kinetic chain exercises may provide more benefit compared to open kinetic chain exercises for some patellofemoral pain syndrome symptoms.
- Self-rated improvement in persistent groin pain is higher after a clinic-based group exercise program compared to multimodal physiotherapy.
Are Non-Invasive Interventions Effective for the Management of Headaches Associated with Neck Pain?
Furthermore, other non-invasive interventions, as well as non-pharmacological interventions, are also commonly utilized to help treat symptoms of neck pain and headaches associated with neck injuries, such as whiplash, caused by automobile accidents. As mentioned before, whiplash is one of the most common types of neck injuries resulting from auto accidents. Chiropractic care, physical therapy and exercise, can be used to improve the symptoms of neck pain, according to the following research studies.
Abstract
Purpose
To update findings of the 2000–2010 Bone and Joint Decade Task Force on Neck Pain and its Associated Disorders and evaluate the effectiveness of non-invasive and non-pharmacological interventions for the management of patients with headaches associated with neck pain (i.e., tension-type, cervicogenic, or whiplash-related headaches).
Methods
We searched five databases from 1990 to 2015 for randomized controlled trials (RCTs), cohort studies, and case–control studies comparing non-invasive interventions with other interventions, placebo/sham, or no interventions. Random pairs of independent reviewers critically appraised eligible studies using the Scottish Intercollegiate Guidelines Network criteria to determine scientific admissibility. Studies with a low risk of bias were synthesized following best evidence synthesis principles.
Results
We screened 17,236 citations, 15 studies were relevant, and 10 had a low risk of bias. The evidence suggests that episodic tension-type headaches should be managed with low load endurance craniocervical and cervicoscapular exercises. Patients with chronic tension-type headaches may also benefit from low load endurance craniocervical and cervicoscapular exercises; relaxation training with stress coping therapy; or multimodal care that includes spinal mobilization, craniocervical exercises, and postural correction. For cervicogenic headaches, low load endurance craniocervical and cervicoscapular exercises; or manual therapy (manipulation with or without mobilization) to the cervical and thoracic spine may also be helpful.

Conclusions
The management of headaches associated with neck pain should include exercise. Patients who suffer from chronic tension-type headaches may also benefit from relaxation training with stress coping therapy or multimodal care. Patients with cervicogenic headache may also benefit from a course of manual therapy.
Keywords
Non-invasive interventions, Tension-type headache, Cervicogenic headache, Headache attributed to whiplash injury, Systematic review
Notes
Acknowledgments
We would like to acknowledge and thank all of the individuals who have made important contributions to this review: Robert Brison, Poonam Cardoso, J. David Cassidy, Laura Chang, Douglas Gross, Murray Krahn, Michel Lacerte, Gail Lindsay, Patrick Loisel, Mike Paulden, Roger Salhany, John Stapleton, Angela Verven, and Leslie Verville. We would also like to thank Trish Johns-Wilson at the University of Ontario Institute of Technology for her review of the search strategy.
Compliance with Ethical Standards
Conflict of Interest
Dr. Pierre Côté has received a grant from the Ontario government, Ministry of Finance, funding from the Canada Research Chairs program, personal fees from National Judicial Institute for lecturing, and personal fees from European Spine Society for teaching. Drs. Silvano Mior and Margareta Nordin have received reimbursement for travel expenses to attend meetings for the study. The remaining authors report no declarations of interest.
Funding
This work was supported by the Ontario Ministry of Finance and the Financial Services Commission of Ontario [RFP# OSS_00267175]. The funding agency had no involvement in the study design, collection, analysis, interpretation of data, writing of the manuscript or decision to submit the manuscript for publication. The research was undertaken, in part, thanks to funding from the Canada Research Chairs program to Dr. Pierre Côté, Canada Research Chair in Disability Prevention and Rehabilitation at the University of Ontario Institute of Technology.
In conclusion, exercise included in chiropractic care and other non-invasive interventions should be utilized as an essential part of treatment to further help improve the symptoms of neck injury as well as that of hip, thigh and knee injury. According to the above research studies, exercise, or physical activity, is beneficial towards speeding up recovery time for patients with automobile accident injuries and for restoring strength, flexibility and mobility to the affected structures of the spine. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
1. Lambers K, Ootes D, Ring D. Incidence of patients with lower
extremity injuries presenting to US emergency departments by
anatomic region, disease category, and age. Clin Orthop Relat
Res 2012;470(1):284-90.
2. Workplace Safety and Insurance Board. By the numbers: 2014
WSIB statistical report. Injury profile—schedule 1; historical
and supplementary data on leading part of body injuries.
[cited June 22, 2015]; Available from: http://www.
wsibstatistics.ca/en/s1injury/s1part-of-body/ 2014.
3. Hincapie CA, Cassidy JD, Côté P, Carroll LJ, Guzman J.
Whiplash injury is more than neck pain: a population-based
study of pain localization after traffic injury. J Occup Environ
Med 2010;52(4):434-40.
4. Bureau of Labor Statistics US Department of Labor. Nonfatal
occupational injuries and illnesses requiring days away from
work. Table 5. Washington, DC 2014 [June 22, 2015];
Available from: http://www.bls.gov/news.release/archives/
osh2_12162014.pdf 2013.
5. New ZealandGuidelinesDevelopmentGroup. The diagnosis and
management of soft tissue knee injuries: internal derangements.
Best practice evidence-based guideline. Wellington: Accident
Compensation Corporation; 2003 [[June 22, 2015]; Available
from: http://www.acc.co.nz/PRD_EXT_CSMP/groups/
external_communications/documents/guide/wcmz002488.pdf].
6. Bizzini M, Childs JD, Piva SR, Delitto A. Systematic review of
the quality of randomized controlled trials for patellofemoral pain
syndrome. J Orthop Sports Phys Ther 2003;33(1):4-20.
7. Crossley K, Bennell K, Green S, McConnell J. A systematic
review of physical interventions for patellofemoral pain
syndrome. Clin J Sport Med 2001;11(2):103-10.
8. Harvie D, O’Leary T, Kumar S. A systematic review of
randomized controlled trials on exercise parameters in the
treatment of patellofemoral pain: what works? J Multidiscip
Healthc 2011;4:383-92.
9. Lepley AS, Gribble PA, Pietrosimone BG. Effects of electromyographic
biofeedback on quadriceps strength: a systematic
review. J Strength Cond Res 2012;26(3):873-82.
10. Peters JS, Tyson NL. Proximal exercises are effective in treating
patellofemoral pain syndrome: a systematic review. Int J Sports
Phys Ther 2013;8(5):689-700.
11. Wasielewski NJ, Parker TM, Kotsko KM. Evaluation of
electromyographic biofeedback for the quadriceps femoris: a
systematic review. J Athl Train 2011;46(5):543-54.
12. Kristensen J, Franklyn-Miller A. Resistance training in musculoskeletal
rehabilitation: a systematic review. Br J Sports Med
2012;46(10):719-26.
13. Larsson ME, Kall I, Nilsson-Helander K. Treatment of patellar
tendinopathy—a systematic review of randomized controlled
trials. Knee Surg Sports Traumatol Arthrosc 2012;20(8):1632-46.
14. Malliaras P, Barton CJ, Reeves ND, Langberg H. Achilles and
patellar tendinopathy loading programmes: a systematic review
comparing clinical outcomes and identifying potential mechanisms
for effectiveness. Sports Med 2013;43(4):267-86.
15. Wasielewski NJ, KotskoKM. Does eccentric exercise reduce pain
and improve strength in physically active adults with symptomatic
lower extremity tendinosis? A systematic review. J Athl Train
2007;42(3):409-21.
16. Reurink G, Goudswaard GJ, Tol JL, Verhaar JA, Weir A, Moen
MH. Therapeutic interventions for acute hamstring injuries: a
systematic review. Br J Sports Med 2012;46(2):103-9.
17. American Academy of Orthopaedic Surgeons. Sprains, strains,
and other soft-tissue injuries. [updated July 2007 March 11,
2013]; Available from: http://orthoinfo.aaos.org/topic.cfm?topic=
A00304 2007.
18. Abenhaim L, Rossignol M, Valat JP, et al. The role of activity in
the therapeutic management of back pain. Report of
the International Paris Task Force on Back Pain. Spine 2000;
25(4 Suppl):1S-33S.
19. McGowan J, Sampson M, Lefebvre C. An evidence
based checklist for the Peer Review of Electronic Search Strategies
(PRESS EBC). Evid Based Library Inf Pract 2010;5(1):149-54.
20. Sampson M, McGowan J, Cogo E, Grimshaw J, Moher D,
Lefebvre C. An evidence-based practice guideline for the peer
review of electronic search strategies. J Clin Epidemiol 2009;
62(9):944-52.
21. Almeida MO, Silva BN, Andriolo RB, Atallah AN, Peccin MS.
Conservative interventions for treating exercise-related musculotendinous,
ligamentous and osseous groin pain. Cochrane
Database Syst Rev 2013;6:CD009565.
22. Ellis R, Hing W, Reid D. Iliotibial band friction syndrome—a
systematic review. Man Ther 2007;12(3):200-8.
23. Machotka Z, Kumar S, Perraton LG. A systematic review of the
literature on the effectiveness of exercise therapy for groin pain in
athletes. SportsMed Arthrosc Rehabil Ther Technol 2009;1(1):5.
24. Moksnes H, Engebretsen L, Risberg MA. The current evidence
for treatment of ACL injuries in children is low: a systematic
review. J Bone Joint Surg Am 2012;94(12):1112-9.
25. Harbour R, Miller J. A new system for grading recommendations
in evidence based guidelines. BMJ 2001;323(7308):
334-6.
26. Carroll LJ, Cassidy JD, Peloso PM, Garritty C, Giles-Smith L.
Systematic search and review procedures: results of the WHO
Collaborating Centre Task Force on Mild Traumatic Brain
Injury. J Rehabil Med 2004(43 Suppl):11-4.
27. Carroll LJ, Cassidy JD, Peloso PM, et al. Methods for the best
evidence synthesis on neck pain and its associated disorders: the
Bone and Joint Decade 2000-2010 Task Force on Neck Pain
and Its Associated Disorders. JManipulative Physiol Ther 2009;
32(2 Suppl):S39-45.
28. Côté P, Cassidy JD, Carroll L, Frank JW, Bombardier C. A
systematic review of the prognosis of acute whiplash and a new
conceptual framework to synthesize the literature. Spine (Phila
Pa 1976) 2001;26(19):E445-58.
29. Hayden JA, Cote P, Bombardier C. Evaluation of the quality of
prognosis studies in systematic reviews. Ann Intern Med 2006;
144(6):427-37.
30. Hayden JA, van der Windt DA, Cartwright JL, Cote P,
Bombardier C. Assessing bias in studies of prognostic factors.
Ann Intern Med 2013;158(4):280-6.
31. Spitzer WO, Skovron ML, Salmi LR, et al. Scientific
monograph of the Quebec Task Force on Whiplash-Associated
Disorders: redefining “whiplash” and its management. Spine
1995;20(8 Suppl):1S-73S.
32. van der Velde G, van Tulder M, Cote P, et al. The sensitivity of
review results to methods used to appraise and incorporate trial
quality into data synthesis. Spine (Phila Pa 1976) 2007;32(7):
796-806.
33. Slavin RE. Best evidence synthesis: an intelligent alternative to
meta-analysis. J Clin Epidemiol 1995;48(1):9-18.
34. Hinman RS, McCrory P, Pirotta M, et al. Efficacy of
acupuncture for chronic knee pain: protocol for a randomised
controlled trial using a Zelen design. BMCComplement Altern
Med 2012;12:161.
35. Crossley KM, Bennell KL, Cowan SM, Green S. Analysis of
outcome measures for persons with patellofemoral pain: which
are reliable and valid? Arch Phys Med Rehabil 2004;85(5):
815-22.
36. Cohen J. A coefficient of agreement for nominal scales. Educ
Psychol Meas 1960;20(1):37-46.
37. Abrams KR, Gillies CL, Lambert PC. Meta-analysis of
heterogeneously reported trials assessing change from baseline.
Stat Med 2005;24(24):3823-44.
38. Follmann D, Elliott P, Suh I, Cutler J. Variance imputation for
overviews of clinical trials with continuous response. J Clin
Epidemiol 1992;45(7):769-73.
39. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred
reporting items for systematic reviews and meta-analyses: the
PRISMA statement. BMJ 2009;339:b2535.
40. Askling CM, Tengvar M, Thorstensson A. Acute hamstring
injuries in Swedish elite football: a prospective randomised
controlled clinical trial comparing two rehabilitation protocols.
Br J Sports Med 2013;47(15):953-9.
41. Dursun N, Dursun E, Kilic Z. Electromyographic biofeedbackcontrolled
exercise versus conservative care for patellofemoral
pain syndrome. Arch Phys Med Rehabil 2001;82(12):1692-5.
42. Harrison EL, Sheppard MS, McQuarry AM. A randomized
controlled trial of physical therapy treatment programs in
patellofemoral pain syndrome. Physiother Can 1999;1999:93-100.
43. Holmich P, Uhrskou P, Ulnits L, et al. Effectiveness of active
physical training as treatment for long-standing adductor-related
groin pain in athletes: randomised trial. Lancet 1999;353(9151):
439-43.
44. Lun VM, Wiley JP, Meeuwisse WH, Yanagawa TL. Effectiveness
of patellar bracing for treatment of patellofemoral pain
syndrome. Clin J Sport Med 2005;15(4):235-40.
45. Malliaropoulos N, Papalexandris S, Papalada A, Papacostas E.
The role of stretching in rehabilitation of hamstring injuries: 80
athletes follow-up. Med Sci Sports Exerc 2004;36(5):756-9.
46. van Linschoten R, van Middelkoop M, Berger MY, et al.
Supervised exercise therapy versus usual care for patellofemoral
pain syndrome: an open label randomised controlled trial. BMJ
2009;339:b4074.
47. Witvrouw E, Cambier D, Danneels L, et al. The effect of exercise
regimens on reflex response time of the vasti muscles in patients
with anterior knee pain: a prospective randomized intervention
study. Scand J Med Sci Sports 2003;13(4):251-8.
48. Witvrouw E, Lysens R, Bellemans J, Peers K, Vanderstraeten G.
Open versus closed kinetic chain exercises for patellofemoral
pain. A prospective, randomized study. Am J Sports Med 2000;
28(5):687-94.
49. Johnson AP, Sikich NJ, Evans G, et al. Health technology
assessment: a comprehensive framework for evidence-based
recommendations in Ontario. Int J Technol Assess Health Care
2009;25(2):141-50.
1.
Carroll LJ, Cassidy JD, Cote P (2006) Frequency, timing, and course of depressive symptomatology after whiplash. Spine 31(16):E551–E556. doi: 10.1097/01.brs.0000225979.26966.9e
CrossRefPubMedGoogle Scholar
2.
Carroll LJ, Liu Y, Holm LW, Cassidy JD, Cote P (2011) Pain-related emotions in early stages of recovery in whiplash-associated disorders: their presence, intensity, and association with pain recovery. Psychosom Med 73(8):708–715. doi: 10.1097/PSY.0b013e31822f991a
CrossRefPubMedGoogle Scholar
3.
Hincapie CA, Cassidy JD, Cote P, Carroll LJ, Guzman J (2010) Whiplash injury is more than neck pain: a population-based study of pain localization after traffic injury. J Occup Environ Med 52(4):434–440. doi: 10.1097/JOM.0b013e3181bb806d
CrossRefPubMedGoogle Scholar
4.
Haldeman S, Carroll LJ, Cassidy JD (2008) The empowerment of people with neck pain: introduction: the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. Spine 33(4 Suppl):S8–S13. doi: 10.1097/BRS.0b013e3181643f51
CrossRefPubMedGoogle Scholar
5.
Cote P, Cassidy JD, Carroll L (2000) The factors associated with neck pain and its related disability in the Saskatchewan population. Spine 25(9):1109–1117
CrossRefPubMedGoogle Scholar
6.
Hagen K, Einarsen C, Zwart JA, Svebak S, Bovim G (2002) The co-occurrence of headache and musculoskeletal symptoms amongst 51 050 adults in Norway. Eur J Neurol 9(5):527–533
CrossRefPubMedGoogle Scholar
7.
Cassidy JD, Carroll LJ, Cote P, Lemstra M, Berglund A, Nygren A (2000) Effect of eliminating compensation for pain and suffering on the outcome of insurance claims for whiplash injury. N Engl J Med 342(16):1179–1186. doi: 10.1056/nejm200004203421606
CrossRefPubMedGoogle Scholar
8.
The international classification of headache disorders, 2nd edition (2004). Cephalalgia 24 (1):1–151. doi: 10.1177/0333102413485658
9.
Posadzki P, Ernst E (2012) Spinal manipulations for tension-type headaches: a systematic review of randomized controlled trials. Complement Ther Med 20(4):232–239
CrossRefPubMedGoogle Scholar
10.
Jensen R, Stovner LJ (2008) Epidemiology and comorbidity of headache. Lancet Neurol 7(4):354–361. doi: 10.1016/s1474-4422(08)70062-0
CrossRefPubMedGoogle Scholar
11.
Ertas M, Baykan B, Orhan EK, Zarifoglu M, Karli N, Saip S, Onal AE, Siva A (2012) One-year prevalence and the impact of migraine and tension-type headache in Turkey: a nationwide home-based study in adults. J Headache Pain 13(2):147–157. doi: 10.1007/s10194-011-0414-5
CrossRefPubMedPubMedCentralGoogle Scholar
12.
Andersen LL, Mortensen OS, Zebis MK, Jensen RH, Poulsen OM (2011) Effect of brief daily exercise on headache among adults—secondary analysis of a randomized controlled trial. Scand J Work Environ Health 37(6):547–550. doi: 10.5271/sjweh.3170
CrossRefPubMedGoogle Scholar
13.
Nilsson N (1995) The prevalence of cervicogenic headache in a random population sample of 20–59 year olds. Spine 20(17):1884–1888
CrossRefPubMedGoogle Scholar
14.
Hurwitz EL, Carragee EJ, van der Velde G, Carroll LJ, Nordin M, Guzman J, Peloso PM, Holm LW, Cote P, Hogg-Johnson S, Cassidy JD, Haldeman S (2009) Treatment of neck pain: noninvasive interventions: results of the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. J Manip Physiol Ther 32(2 Suppl):S141–S175. doi: 10.1016/j.jmpt.2008.11.017
CrossRefGoogle Scholar
15.
Jull G, Trott P, Potter H, Zito G, Niere K, Shirley D, Emberson J, Marschner I, Richardson C (2002) A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache. Spine 27(17):1835–1843 (discussion 1843)
CrossRefPubMedGoogle Scholar
16.
Carroll LJ, Hurwitz EL, Cote P, Hogg-Johnson S, Carragee EJ, Nordin M, Holm LW, van der Velde G, Cassidy JD, Guzman J, Peloso PM, Haldeman S (2009) Research priorities and methodological implications: the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. J Manip Physiol Ther 32(2 Suppl):S244–S251. doi: 10.1016/j.jmpt.2008.11.024
CrossRefGoogle Scholar
17.
Sjaastad O, Fredriksen TA, Pfaffenrath V (1998) Cervicogenic headache: diagnostic criteria. The cervicogenic headache international study group. Headache 38(6):442–445
CrossRefPubMedGoogle Scholar
18.
Aker PD, Gross AR, Goldsmith CH, Peloso P (1996) Conservative management of mechanical neck pain: systematic overview and meta-analysis. BMJ 313(7068):1291–1296
CrossRefPubMedPubMedCentralGoogle Scholar
19.
van Tulder MW, Koes BW, Bouter LM (1997) Conservative treatment of acute and chronic nonspecific low back pain. A systematic review of randomized controlled trials of the most common interventions. Spine (Phila Pa 1976) 22(18):2128–2156
CrossRefGoogle Scholar
20.
Norman GR, Streiner DL (2008) Biostatistics: the bare essentials, 3rd edn. BC Decker, Hamilton
Google Scholar
21.
Sampson M, McGowan J, Cogo E, Grimshaw J, Moher D, Lefebvre C (2009) An evidence-based practice guideline for the peer review of electronic search strategies. J Clin Epidemiol 62(9):944–952. doi: 10.1016/j.jclinepi.2008.10.012
CrossRefPubMedGoogle Scholar
22.
McGowan J, Sampson M, Lefebvre C (2010) An evidence based checklist for the peer review of electronic search strategies (PRESS EBC). Evid Based Libr Inf Pract 5(1):149–154
CrossRefGoogle Scholar
23.
Harbour R, Miller J (2001) A new system for grading recommendations in evidence based guidelines. BMJ 323(7308):334–336. doi: 10.1136/bmj.323.7308.334
CrossRefPubMedPubMedCentralGoogle Scholar
24.
van der Velde G, van Tulder M, Côté P, Hogg-Johnson S, Aker P, Cassidy JD, Carragee E, Carroll L, Guzman J, Haldeman S, Holm L, Hurwitz E, Nordin M, Peloso P (2007) The sensitivity of review results to methods used to appraise and incorporate trial quality into data synthesis. Spine (Phila Pa 1976) 32(7):796–806. doi: 10.1097/01.brs.0000258903.67718.d5
CrossRefGoogle Scholar
25.
Spitzer WO, Skovron ML, Salmi LR, Cassidy JD, Duranceau J, Suissa S, Zeiss E (1995) Scientific monograph of the Quebec task force on whiplash-associated disorders: redefining “whiplash” and its management. Spine 20(8 Suppl):1S–73S
PubMedGoogle Scholar
26.
Carroll LJ, Cassidy JD, Peloso PM, Giles-Smith L, Cheng CS, Greenhalgh SW, Haldeman S, van der Velde G, Hurwitz EL, Cote P, Nordin M, Hogg-Johnson S, Holm LW, Guzman J, Carragee EJ (2009) Methods for the best evidence synthesis on neck pain and its associated disorders: the bone and joint decade 2000–2010 task force on neck pain and its associated disorders. J Manip Physiol Ther 32(2 Suppl):S39–S45. doi: 10.1016/j.jmpt.2008.11.009
CrossRefGoogle Scholar
27.
Carroll LJ, Cassidy JD, Peloso PM, Garritty C, Giles-Smith L (2004) Systematic search and review procedures: results of the WHO Collaborating centre task force on mild traumatic brain injury. J Rehabil Med (43 Suppl):11–14
Google Scholar
28.
Cote P, Cassidy JD, Carroll L, Frank JW, Bombardier C (2001) A systematic review of the prognosis of acute whiplash and a new conceptual framework to synthesize the literature. Spine 26(19):E445–E458
CrossRefPubMedGoogle Scholar
29.
Hayden JA, Cote P, Bombardier C (2006) Evaluation of the quality of prognosis studies in systematic reviews. Ann Intern Med 144(6):427–437
CrossRefPubMedGoogle Scholar
30.
Hayden JA, van der Windt DA, Cartwright JL, Cote P, Bombardier C (2013) Assessing bias in studies of prognostic factors. Ann Intern Med 158(4):280–286. doi: 10.7326/0003-4819-158-4-201302190-00009
CrossRefPubMedGoogle Scholar
31.
Slavin RE (1995) Best evidence synthesis: an intelligent alternative to meta-analysis. J Clin Epidemiol 48(1):9–18
CrossRefPubMedGoogle Scholar
32.
Stauffer ME, Taylor SD, Watson DJ, Peloso PM, Morrison A (2011) Definition of nonresponse to analgesic treatment of arthritic pain: an analytical literature review of the smallest detectable difference, the minimal detectable change, and the minimal clinically important difference on the pain visual analog scale. Int J Inflam 2011:231926. doi: 10.4061/2011/231926
CrossRefPubMedPubMedCentralGoogle Scholar
33.
Carroll LJ, Jones DC, Ozegovic D, Cassidy JD (2012) How well are you recovering? The association between a simple question about recovery and patient reports of pain intensity and pain disability in whiplash-associated disorders. Disabil Rehabil 34(1):45–52. doi: 10.3109/09638288.2011.587085
CrossRefPubMedGoogle Scholar
34.
Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole RM (2001) Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 94(2):149–158
CrossRefPubMedGoogle Scholar
35.
McCarthy MJ, Grevitt MP, Silcocks P, Hobbs G (2007) The reliability of the Vernon and Mior neck disability index, and its validity compared with the short form-36 health survey questionnaire. Eur Spine J 16(12):2111–2117. doi: 10.1007/s00586-007-0503-y
CrossRefPubMedPubMedCentralGoogle Scholar
36.
Sim J, Jordan K, Lewis M, Hill J, Hay EM, Dziedzic K (2006) Sensitivity to change and internal consistency of the northwick park neck pain questionnaire and derivation of a minimal clinically important difference. Clin J Pain 22(9):820–826. doi: 10.1097/01.ajp.0000210937.58439.39
CrossRefPubMedGoogle Scholar
37.
Lauche R, Langhorst J, Dobos GJ, Cramer H (2013) Clinically meaningful differences in pain, disability and quality of life for chronic nonspecific neck pain—a reanalysis of 4 randomized controlled trials of cupping therapy. Complement Ther Med 21(4):342–347. doi: 10.1016/j.ctim.2013.04.005
CrossRefPubMedGoogle Scholar
38.
Abrams KR, Gillies CL, Lambert PC (2005) Meta-analysis of heterogeneously reported trials assessing change from baseline. Stat Med 24(24):3823–3844. doi: 10.1002/sim.2423
CrossRefPubMedGoogle Scholar
39.
Follmann D, Elliott P, Suh I, Cutler J (1992) Variance imputation for overviews of clinical trials with continuous response. J Clin Epidemiol 45(7):769–773
CrossRefPubMedGoogle Scholar
40.
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6(7):e1000097. doi: 10.1371/journal.pmed.1000097
CrossRefPubMedPubMedCentralGoogle Scholar
41.
Bove G, Nilsson N (1998) Spinal manipulation in the treatment of episodic tension-type headache: a randomized controlled trial. JAMA J Am Med Assoc 280(18):1576–1579
CrossRefGoogle Scholar
42.
Castien RF, van der Windt DA, Grooten A, Dekker J (2011) Effectiveness of manual therapy for chronic tension-type headache: a pragmatic, randomised, clinical trial. Cephalalgia 31(2):133–143. doi: 10.1177/0333102410377362
CrossRefPubMedGoogle Scholar
43.
Endres HG, Bowing G, Diener HC, Lange S, Maier C, Molsberger A, Zenz M, Vickers AJ, Tegenthoff M (2007) Acupuncture for tension-type headache: a multicentre, sham-controlled, patient-and observer-blinded, randomised trial. J Headache Pain 8(5):306–314. doi: 10.1007/s10194-007-0416-5
CrossRefPubMedPubMedCentralGoogle Scholar
44.
Haas M, Spegman A, Peterson D, Aickin M, Vavrek D (2010) Dose response and efficacy of spinal manipulation for chronic cervicogenic headache: a pilot randomized controlled trial. Spine J Off J N Am Spine Soc 10(2):117–128. doi: 10.1016/j.spinee.2009.09.002
CrossRefGoogle Scholar
45.
Haas M, Schneider M, Vavrek D (2010) Illustrating risk difference and number needed to treat from a randomized controlled trial of spinal manipulation for cervicogenic headache. Chiropr Osteopat 18:9. doi: 10.1186/1746-1340-18-9
CrossRefPubMedPubMedCentralGoogle Scholar
46.
Holroyd KA, O’Donnell FJ, Stensland M, Lipchik GL, Cordingley GE, Carlson BW (2001) Management of chronic tension-type headache with tricyclic antidepressant medication, stress management therapy, and their combination: a randomized controlled trial. JAMA J Am Med Assoc 285(17):2208–2215
CrossRefGoogle Scholar
47.
Jena S, Witt CM, Brinkhaus B, Wegscheider K, Willich SN (2008) Acupuncture in patients with headache. Cephalalgia 28(9):969–979. doi: 10.1111/j.1468-2982.2008.01640.x
CrossRefPubMedGoogle Scholar
48.
Melchart D, Streng A, Hoppe A, Brinkhaus B, Witt C, Wagenpfeil S, Pfaffenrath V, Hammes M, Hummelsberger J, Irnich D, Weidenhammer W, Willich SN, Linde K (2005) Acupuncture in patients with tension-type headache: randomised controlled trial. BMJ 331(7513):376–382. doi: 10.1136/bmj.38512.405440.8F
CrossRefPubMedPubMedCentralGoogle Scholar
49.
Soderberg E, Carlsson J, Stener-Victorin E (2006) Chronic tension-type headache treated with acupuncture, physical training and relaxation training. Between-group differences. Cephalalgia 26(11):1320–1329. doi: 10.1111/j.1468-2982.2006.01209.x
CrossRefPubMedGoogle Scholar
50.
Soderberg EI, Carlsson JY, Stener-Victorin E, Dahlof C (2011) Subjective well-being in patients with chronic tension-type headache: effect of acupuncture, physical training, and relaxation training. Clin J Pain 27(5):448–456. doi: 10.1097/AJP.0b013e318208c8fe
CrossRefPubMedGoogle Scholar
51.
van Ettekoven H, Lucas C (2006) Efficacy of physiotherapy including a craniocervical training programme for tension-type headache; a randomized clinical trial. Cephalalgia 26(8):983–991. doi: 10.1111/j.1468-2982.2006.01163.x
CrossRefPubMedGoogle Scholar
52.
Boline PD, Kassak K, Bronfort G, Nelson C, Anderson AV (1995) Spinal manipulation vs. amitriptyline for the treatment of chronic tension-type headaches: a randomized clinical trial. J Manip Physiol Ther 18(3):148–154
Google Scholar
53.
Carlsson J, Fahlcrantz A, Augustinsson LE (1990) Muscle tenderness in tension headache treated with acupuncture or physiotherapy. Cephalalgia 10(3):131–141
CrossRefPubMedGoogle Scholar
54.
Carlsson J, Augustinsson LE, Blomstrand C, Sullivan M (1990) Health status in patients with tension headache treated with acupuncture or physiotherapy. Headache 30(9):593–599
CrossRefPubMedGoogle Scholar
55.
Karst M, Reinhard M, Thum P, Wiese B, Rollnik J, Fink M (2001) Needle acupuncture in tension-type headache: a randomized, placebo-controlled study. Cephalalgia 21(6):637–642
CrossRefPubMedGoogle Scholar
56.
Mousavi SA, Mirbod SM, Khorvash F (2011) Comparison between efficacy of imipramine and transcutaneous electrical nerve stimulation in the prophylaxis of chronic tension-type headache: a randomized controlled clinical trial. J Res Med Sci 16(7):923–927
PubMedPubMedCentralGoogle Scholar
57.
Bellamy R (2004) An introduction to patient education: theory and practice. Med Teach 26(4):359–365. doi: 10.1080/01421590410001679398
CrossRefPubMedGoogle Scholar
58.
Group AAMPG (2003) Evidence-based management of acute musculoskeletal pain
Google Scholar
59.
Abenhaim L, Rossignol M, Valat JP, Nordin M, Avouac B, Blotman F et al. (2000) The role of activity in the therapeutic management of back pain. Report of the International Paris Task Force on Back Pain. Spine (Phila Pa 1976) 25(4 Suppl):1S–33S
Google Scholar
60.
Rubinstein SM, Terwee CB, Assendelft WJ, de Boer MR, van Tulder MW (2012) Spinal manipulative therapy for acute low-back pain. Cochrane Database Syst Rev 9:CD008880. doi: 10.1002/14651858.CD008880.pub2
PubMedGoogle Scholar
61.
Maitland G, Hengeveld E, Banks K, English K (2005) Maitland’s Vertebral Manipulation, 7 edn. Elsevier Butterworth Heinemann, Toronto
Google Scholar
62.
Peake N, Harte A (2005) The effectiveness of cervical traction. Phys Ther Rev 10:217–229
CrossRefGoogle Scholar
63.
Graham N, Gross AR, Goldsmith C (2006) Mechanical traction for mechanical neck disorders: a systematic review. J Rehabil Med 38(3):145–152. doi: 10.1080/16501970600583029
CrossRefPubMedGoogle Scholar
64.
World Health Organization (2002) Acupuncture: review and analysis of reports on controlled clinical trials. World Health Organization, Geneva
Google Scholar
65.
Aas RW, Tuntland H, Holte KA, Roe C, Lund T, Marklund S et al. (2011) Workplace interventions for neck pain in workers. Cochrane Database Syst Rev (4):CD008160. doi: 10.1002/14651858.CD008160.pub2
66.
Burns JW, Higdon LJ, Mullen JT, Lansky D, Wei JM (1999) Relationships among patient hostility, anger expression, depression, and the working alliance in a work hardening program. Ann Behav Med 21(1):77–82. doi: 10.1007/bf02895037
CrossRefPubMedGoogle Scholar
67.
Schaafsma F, Schonstein E, Ojajarvi A, Verbeek J (2011) Physical conditioning programs for improving work outcomes among workers with back pain. Scand J Work Environ Health 37(1):1–5
CrossRefPubMedGoogle Scholar
68.
Gardner BT, Pransky G, Shaw WS, Nha Hong Q, Loisel P (2010) Researcher perspectives on competencies of return-to-work coordinators. Disabil Rehabil 32(1):72–78. doi: 10.3109/09638280903195278
CrossRefPubMedGoogle Scholar
69.
Shaw W, Hong QN, Pransky G, Loisel P (2008) A literature review describing the role of return-to-work coordinators in trial programs and interventions designed to prevent workplace disability. J Occup Rehabil 18(1):2–15. doi: 10.1007/s10926-007-9115-y
CrossRefPubMedGoogle Scholar
70.
Driessen MT, Proper KI, van Tulder MW, Anema JR, Bongers PM, van der Beek AJ (2010) The effectiveness of physical and organisational ergonomic interventions on low back pain and neck pain: a systematic review. Occup Environ Med 67(4):277–285. doi: 10.1136/oem.2009.047548
CrossRefPubMedGoogle Scholar

Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.

IMPORTANT TOPIC: EXTRA EXTRA: Treating Sciatica Pain
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card