


Benign Paroxysmal Positional Vertigo, or BPPV, is the most common vestibular disorder and it is by far the most common cause of vertigo, a false sensation of rotational movement or spinning. BPPV isn’t life-threatening, it can come in unexpectedly in brief spells and it can trigger with certain head positions or motions. This might frequently occur when you tip your head down or up, when you lie down, or when you flip over or sit up in bed.
BPPV is a mechanical problem in the inner ear. It occurs when some of the calcium carbonate crystals, known as otoconia, that are typically embedded in gel at the utricle, become dislodged and migrate into at least one of the 3 fluid-filled semicircular canals, in which they are not supposed to be. When enough of these particles collect among the canals, they interfere with the fluid movement that these canals use to sense head motion, causing the internal ear to send false signals to the brain.
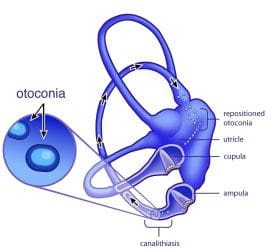
Fluid from the canals does not normally respond to gravity. On the other hand, the crystals do interact with gravity, thereby shifting the fluid when it normally would remain still. After the fluid moves, nerve endings in the canal are triggered and send a message to the brain that the head is moving, even though it is not. This false information does not match what the other ear may be sensing, together with what the eyes are seeing, or using what the muscles and joints do, and this mismatched information is sensed by the brain as a spinning sensation, or vertigo, which normally lasts less than one minute. Between vertigo spells some people may feel symptom-free, while others feel a mild sense of imbalance or disequilibrium.
Table of Contents
Symptoms of BPPV
The signs and symptoms of benign paroxysmal positional vertigo, or BPPV, may include:
- Dizziness
- A feeling that you or your surroundings are spinning or moving (vertigo)
- A loss of equilibrium or balance
- Nausea
- Vomiting
The signs and symptoms of BPPV can come and go, with these generally lasting less than one minute. Episodes of benign paroxysmal positional vertigo can disappear for a while and then return. Activities that cause the signs and symptoms of BPPV may vary from person to person, but are nearly always brought on by a change in the placement of the head. Some people also feel out of balance when standing or walking. Abnormal rhythmic eye movements, known as nystagmus, usually follow the outward signs of benign paroxysmal positional vertigo, or BPPV.
It’s essential, however, to understand that BPPV will not give you continuous dizziness that is unaffected by motion or even a change in position. Also, it will not affect your hearing or produce fainting, headache or neurological signs, such as numbness, a sensation of “pins and needles,” difficulty speaking or difficulty coordinating your movements. If you have one or more of these additional symptoms, tell a healthcare professional immediately. Other disorders could be originally misdiagnosed as BPPV. By alerting a healthcare professional about any signs and symptoms you may be experiencing along with vertigo, they could reevaluate your illness and think about whether you might have another kind of disorder, instead of or in addition to BPPV.
BPPV is rather common, with an estimated prevalence of 107 per 100,000 annually plus a lifetime prevalence of 2.4 percent. It is thought to be quite rare in children but can affect adults of any age, particularly seniors. The wide majority of cases happen for no apparent reason, with many individuals describing how they simply went to get out of bed and the room began to spin. Nevertheless, associations have been made with injury, migraine headaches, inner ear infection or disease, diabetes, osteoporosis, intubation, presumably due to protracted time lying in bed, and reduced blood flow. There might also be a correlation with a person’s favorite sleeping side.
Diagnosis for BPPV
General practitioners normally refer patients to a healthcare professional specifically trained to take care of vestibular disorders, most commonly a vestibular rehabilitation therapist, such as a chiropractor, a specially trained physical therapist, or sometimes an occupational therapist or audiologist. An ENT (ear, nose & throat specialist) who specializes on vestibular disorders can also diagnose BPPV.
Normal medical imaging (e.g. an MRI) isn’t effective in diagnosing BPPV, because it doesn’t show the crystals that have moved to the semi-circular canals. However, when someone with BPPV has their own head moved into a position that makes the dislodged crystals go within a canal, the error signals have been known to cause the eyes to move in a very specific pattern, known as “nystagmus”.
The association between the internal ears and the eye muscles are what generally permit us to remain focused on our environment while the head is moving. Since the dislodged crystals make the brain think a person is moving when they are not, it causes the eyes to move, making it seem like the room is spinning. The eye movement is the indication that something is happening automatically in order to move the fluid in the inner ear canals when it shouldn’t be.
The nystagmus will have different characteristics that allow a healthcare professional to recognize which ear the displaced crystals are inside, as well as which canal(s) they have moved into. Evaluations like the Dix-Hallpike test involves moving the head into specific orientations, allowing gravity to move the dislodged crystals and activate the vertigo while the healthcare professional watches for the recognizable eye movements, or nystagmus.
Dix-Hallpike Test for BPPV
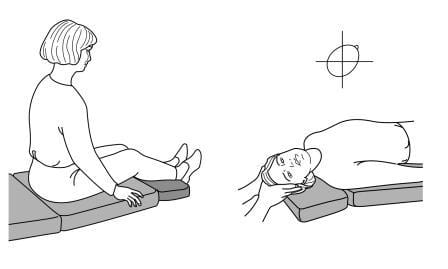
Healthcare professionals, such as chiropractors specializing in vestibular diseases, typically utilize the Dix-Hallpike test, sometimes called the Dix-Hallpike maneuver, to test for benign paroxysmal positional vertigo, or BPPV. To execute the Dix-Hallpike test, your doctor will ask you to sit on the test table with your legs stretched out. He’ll turn your head 45 degrees to one side, which contrasts the right posterior semicircular canal with the sagittal plane of the body, then they are going to allow you to lie back quickly, while the eyes are open, so that your head hangs slightly over the edge of the desk.
Dix-Hallpike Test to Diagnose BPPV
This motion may cause the loose crystals to move inside your semicircular canals. The healthcare professional will ask if you are feeling symptoms of vertigo and observe your eyes to find out how they move. As soon as you’ve got a few minutes to recover, your doctor may do the test on the opposite side of your head.
The latency, length and direction of nystagmus, if present, along with the latency and duration of vertigo, if present, should be noted. If the test is negative, it will demonstrate that benign paroxysmal positional vertigo is a less probable diagnosis and central nervous system involvement ought to be considered. There are two sorts of BPPV: One at which loose crystals can move freely in the fluid of the canal (canalithiasis), and, more infrequently, one where the crystals are believed to be ‘wrapped up’ on the bundle of nerves that feel the fluid motion, or cupulolithiasis.
With canalithiasis, it requires less than a moment for those crystals to stop moving after a particular change in head position has triggered a twist. Once the crystals quit shifting, the fluid motion settles and the nystagmus and vertigo cease. With cupulolithiasis, the crystals trapped on the package of sensory nerves will make the nystagmus and vertigo last longer, until the head is moved out of the offending position. It is necessary to make the proper diagnosis, since the treatment is different for every variant. BPPV can be treated using various treatment methods, one of the most common being the Epley Maneuver.

Dr. Alex Jimenez’s Insight
Chiropractic care is an alternative treatment option commonly utilized to help treat a variety of injuries and conditions associated with the proper alignment of the spine. Occasionally, a spinal misalignment, or subluxation, can develop into numerous health issues, causing a wide array of symptoms if left untreated for an extended period of time. However, many chiropractors can treat many other ailments not closely associated with the spine. In a clinical setting, chiropractic care has been used for the management of benign paroxysmal positional vertigo, or BPPV. Chiropractors will utilize the Dix-Hallpike test to diagnose a patient followed by the Epley maneuver to help treat patients with BPPV. Many patients have reported a reduction in symptoms.
The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez

Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.

Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card