


El Paso, TX. Chiropractor, Dr. Alexander Jimenez looks at childhood developmental disorders, along with their symptoms, causes and treatment.
Table of Contents
Cerebral Palsy
-
4 Types
-
Spastic Cerebral Palsy
- ~80% of CP cases
-
Dyskinetic Cerebral Palsy (also includes athetoid, choreoathetoid, and dystonic cerebral palsies)
-
Ataxic Cerebral Palsy
-
Mixed Cerebral Palsy
Autism Spectrum Disorder
-
Autistic Disorder
-
Asperger’s Disorder
-
Pervasive Developmental Disorder–Not Otherwise Specified (PDD-NOS)
-
Childhood Disintegrative Disorder (CDD)
Autism Spectrum Disorder Red Flags
-
Social Communication
- Limited use of gestures
- Delayed speech or lack of babble
- Odd sounds or unusual tone of voice
- Difficulty making eye contact, gestures and words at the same time
- Little imitation of others
- No longer uses words they used to use
- Uses another person’s hand as a tool
-
Social Interaction
- Difficulty making eye contact
- Lack of joyful expression
- Lack of responsiveness to name
- Does not try to show you things they’re interested in
-
Repetitive Behaviors & Restricted Interests
- Unusual way of moving their hands, fingers or body
- Develops rituals, such as lining up objects or repeating things
- Focuses on unusual objects
- Excessive interest in a particular object or activity which interferes with social interaction
- Unusual sensory interests
- Under or over reaction to sensory input
ASD Diagnostic Criteria (DSM-5)
-
Persistent deficits in social communication and social interaction across multiple contexts, as manifested by the following, currently or by history (examples are illustrative, not exhaustive; see text):
-
Deficits in social-emotional reciprocity, ranging, for example, from abnormal social approach and failure of normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
-
Deficits in nonverbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and use of gestures; to a total lack of facial expressions and nonverbal communication.
-
Deficits in developing, maintaining, and understand relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers.
ASD Diagnostic Criteria
-
Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the following, currently or by history (examples are illustrative, not exhaustive; see text):
-
Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor stereotypes, lining up toys or flipping objects, echolalia, idiosyncratic phrases).
-
Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day).
-
Highly restricted, fixated interests that are abnormal in intensity or focus (e.g., strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).
-
Hyper – or Hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g. apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement).
ASD Diagnostic Criteria
-
Symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life).
-
Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
-
These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism spectrum disorder frequently co-occur; to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level.
ASD Diagnostic Criteria (ICD- 10)
A. Abnormal or impaired development is evident before the age of 3 years in at least one of the following areas:
-
Receptive or expressive language as used in social communication;
-
The development of selective social attachments or of reciprocal social interaction;
-
Functional or symbolic play.
B. A total of at least six symptoms from (1), (2) and (3) must be present, with at least two from (1) and at least one from each of (2) and (3)
1. Qualitative impairment in social interaction are manifest in at least two of the following areas:
a. failure adequately to use eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction;
b. failure to develop (in a manner appropriate to mental age, and despite ample opportunities) peer relationships that involve a mutual sharing of interests, activities and emotions;
c. lack of socio-emotional reciprocity as shown by an impaired or deviant response to other people’s emotions; or lack of modulation of behavior according to
social context; or a weak integration of social, emotional, and communicative behaviors;
d. lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g. a lack of showing, bringing, or pointing out to other people objects of interest to the individual).
2. Qualitative abnormalities in communication as manifest in at least one of the following areas:
a. delay in or total lack of, development of spoken language that is not accompanied by an attempt to compensate through the use of gestures or mime as an alternative mode of communication (often preceded by a lack of communicative babbling);
b. relative failure to initiate or sustain conversational interchange (at whatever level of language skill is present), in which there is reciprocal responsiveness to the communications of the other person;
c. stereotyped and repetitive use of language or idiosyncratic use of words or phrases;
d. lack of varied spontaneous make-believe play or (when young) social imitative play
3. Restricted, repetitive, and stereotyped patterns of behavior, interests, and activities are manifested in at least one of the following:
a. An encompassing preoccupation with one or more stereotyped and restricted patterns of interest that are abnormal in content or focus; or one or more interests that are abnormal in their intensity and circumscribed nature though not in their content or focus;
b. Apparently compulsive adherence to specific, nonfunctional routines or rituals;
c. Stereotyped and repetitive motor mannerisms that involve either hand or finger flapping or twisting or complex whole body movements;
d. Preoccupations with part-objects of non-functional elements of play materials (such as their oder, the feel of their surface, or the noise or vibration they
generate).
C. The clinical picture is not attributable to the other varieties of pervasive developmental disorders; specific development disorder of receptive language (F80.2) with secondary socio-emotional problems, reactive attachment disorder (F94.1) or disinhibited attachment disorder (F94.2); mental retardation (F70-F72) with some associated emotional or behavioral disorders; schizophrenia (F20.-) of unusually early onset; and Rett’s Syndrome (F84.12).
Asperger’s Syndrome Diagnostic Criteria (ICD-10)
-
A. Qualitative impairment in social interaction, as manifested by at least two of the following:
- marked impairments in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction.
- failure to develop peer relationships appropriate to developmental level.
- a lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g. by a lack of showing, bringing, or pointing out objects of interest to other people).
- lack of social or emotional reciprocity.
-
B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following:
- encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus.
- apparently inflexible adherence to specific, nonfunctional routines or rituals.
- stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements).
- persistent preoccupation with parts of objects.
C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning
D. There is no clinically significant general delay in language (e.g., single words used by age 2 years, communicative phrases used by age 3 years).
E. There is no clinically significant delay in cognitive development or in the development of age-appropriate self- help skills, adaptive behavior (other than social interaction), and curiosity about the environment in childhood.
F. Criteria are not met for another specific Pervasive Developmental Disorder or Schizophrenia.
Attention-Deficit/Hyperactivity Disorder (ADHD)
- Inattention – gets off task easily
- Hyperactivity – seems to move about constantly
- Impulsivity – makes hasty actions that occur in the moment without first thinking about them
ADHD Risk Factors
- Genetics
- Cigarette smoking, alcohol use, or drug use during pregnancy
- Exposure to environmental toxins during pregnancy
- Exposure to environmental toxins, such as high levels of lead, at a young age
- Low birth weight
- Brain injuries
Developmental Screening
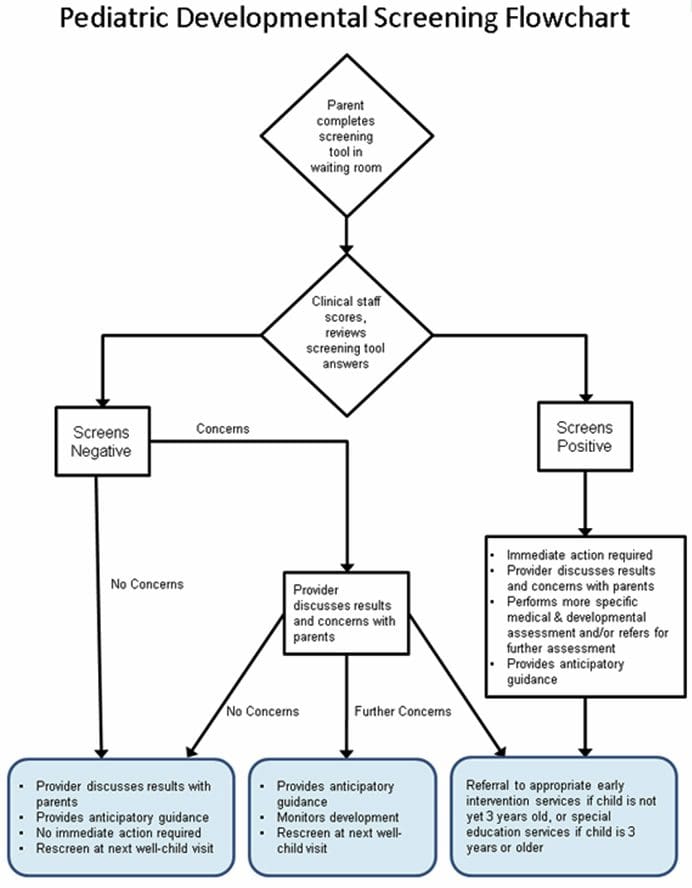
https://www.cdc.gov/ncbddd/autism/hcp- screening.html
Primitive Reflexes
- Moro
- Spinal Galant
- Asymmetrical Tonic Neck Reflex
- Symetrical Tonic Neck Reflex
- Tonic Labrynthine Reflex
- Palmomental Reflex
- Snout Reflex
Treatment Of Developmental Delays
- Remediate any retained reflexes
- Educate parents on providing a structured environment
- Promote brain balancing activities
- Address food sensitivities and remove likely problematic foods
- Treat the patient’s gut – probiotics, glutamine, etc.
Pediatric Acute-Onset Neuropsychiatric Syndrome
(PANS)
-
Abrupt dramatic onset of OCD or severely restricted food intake
-
Symptoms are not better explained by a known neurologic or medical disorder
-
Also at least two of the following:
- Anxiety
- Emotional lability and/or depression
- Irritability, aggression and/or severely oppositional behaviors
- Behavioral/Developmental regression
- Deterioration in school performance
- Sensory or motor abnormalities
- Somatic signs including sleep disturbances, enuresis or urinary frequency
-
*The onset of PANS may start with infectious agents other than strep. It also includes onset from environmental triggers or immune dysfunction
Pediatric Autoimmune Disorders Associated With Streptococcus
(PANDAS)
-
Presence of significant obsessions, compulsions and/or tics
-
Abrupt onset of symptoms or a relapsing-remitting course of symptom severity
-
Pre-pubertal onset
-
Association with streptococcal infection
-
Association with other neuropsychiatric symptoms (including any of the PANS “accompanying” symptoms)
PANS/PANDAS Tests
- Swab/Strep culture
- Blood tests for strep
- Strep ASO
- Anti-DNase B Titer
- Streptozyme
- Test for other infectious agents
- MRI preferred but PET can be used if necessary
- EEG
False Negatives
-
Not all children who have strep have elevated labs
- Only 54% of children with strep showed a significant increase in ASO.
- Only 45% showed an increase in anti–DNase B.
- Only 63% showed an increase in either ASO and/or anti–DNase B.
Treatment Of PANS/PANDAS
- Antibiotics
- IVIG
- Plasmaphoresis
- Anti-Inflammatory protocols
- Steroid medications
- Omega-3’s
- NSAIDS
- Probiotics
Injury Medical Clinic: Chiropractor
Sources
- “Attention Deficit Hyperactivity Disorder.” National Institute of Mental Health, U.S. Department of Health and Human Services, www.nimh.nih.gov/health/topics/attention-deficit-hyperactivity-disorder-adhd/index.shtml.
- Autism Navigator, www.autismnavigator.com/.
“Autism Spectrum Disorder (ASD).” Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 29 May 2018, www.cdc.gov/ncbddd/autism/index.html. - “Introduction to Autism.” Interactive Autism Network, iancommunity.org/introduction-autism.
- Shet, Anita, et al. “Immune Response to Group A Streptococcal C5a Peptidase in Children: Implications for Vaccine Development.” The Journal of Infectious Diseases, vol. 188, no. 6, 2003, pp. 809–817., doi:10.1086/377700.
- “What Is PANDAS?” PANDAS Network, www.pandasnetwork.org/understanding-pandaspans/what-is-pandas/.
Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card