


Active Release Technique (A.R.T) is a hands on soft tissue treatment for ligaments, tendons muscles and nerves. It is the leading soft tissue treatment utilized widely in the treatment of soft tissue injuries and conditions among professional athletes and the general population alike. In the instance of chronic neck pain, along with shoulder and subscapularis pain, ART involves guided pressure being applied to a shortened muscle in the top region of the neck or cervical spine. Most commonly, a healthcare professional will move the patient’s head in a direction that lengthens the muscle. During the motion the doctor maintains a strain on the muscle, as it slides out from beneath the doctor’s fingers.
The active release technique hurts a bit (many patients describe it as a”good hurt”), and it feels like a stretch that you need but can’t do yourself. When a muscle is tight the procedure operates by increasing the nervous system’s tolerance to extend the muscle. ART is utilized to take care of repetitive strain injuries, and it is often used in a variety of other medical practices. This is because it can offer quick results in treating ailments like: tennis elbow, frozen shoulder, shoulder rotator cuff injuries and plantar fasciitis. ART permits the physician to isolate treatment to each individual small muscle of the neck, and treat it through its full selection of movement. The neck muscles are layered, and also to isolate them during therapy demands careful attention.
Table of Contents
Effects of the Active Release Technique on Pain and Range of Motion in Patients with Chronic Neck Pain
Abstract
- Purpose: To compare the influences of the active release technique (ART) and joint mobilization (JM) on the visual analog scale (VAS) pain score, pressure pain threshold (PPT), and neck range of motion (ROM) of patients with chronic neck pain.
- Subjects: Twenty-four individuals with chronic neck pain were randomly and equally assigned to 3 groups: an ART group, a joint mobilization (JM) group, and a control group. Before and after the intervention, the degree of pain, PPT, and ROM of the neck were measured using a VAS, algometer, and goniometer, respectively.
- Results: The ART group and JM group demonstrated significant changes in VAS and ROM between pre and post-intervention, while no significant change was observed in the control group. Significant differences in the PPT of all muscles were found in the ART group, while significant differences in all muscles other than the trapezius were found in the JM group. No significant difference in PPT was observed in any muscle of the control group. The posthoc test indicated no statistically significant difference between the ART and JM group, but the differences of variation in VAS, PPT, and ROM were greater in the ART group than in the JM and control groups.
- Conclusion: ART for the treatment of chronic neck pain may be beneficial for neck pain and movement.
- Key words: Active release technique, Soft tissue, Chronic neck pain
Introduction
People have a 70% likelihood of developing neck pain during their lives; thus, neck pain is an important issue affecting economic productivity in modern society[1]. Neck pain is a work-related musculoskeletal disorder that can occur when a person works for a long time or at a high intensity. An increasing number of patients also visit hospitals complaining of pain occurring not only in the neck but also in the upper extremities and head as a result of sustained excessive tension[2]. Although the issue of neck pain is becoming increasingly common and important, research into optimal treatmentslacking[3].
A common cause of neck pain is mechanical dysfunction, which causes abnormal joint movement, as abnormal cervical joint mobility inside the joint capsule can limit neck movement[4, 5]. Additionally, unbalanced soft tissue around the head and neck structure can place limits on the range of motion (ROM) of the head and cause neck pain[6]. Therefore, many treatments are performed with the aim of restoring soft tissue function or mobility to the joints in patients with chronic neck pain. Joint mobilization (JM) and joint manipulation are the most widely used methods to increase mobility inside the joint capsule. These methods have been reported to increase the ROM and relieve pain[7, 8]. However, JM and joint manipulation performed at the end range of the ROM directly on the joints of the cervical vertebrae can cause tension in the patient’s neck muscles, because the cervical vertebrae are the most sensitive part of the spine and this tension protects the nerves and blood vessels[9].
The active release technique (ART) is a manual therapy for the recovery of soft tissue function that involves the removal of scar tissue, which can cause pain, stiffness, muscle weakness, and abnormal sensations including mechanical dysfunction in the muscles, myofascia, and soft tissue[10]. The effectiveness of ART has been reported for carpal tunnel syndrome, Achilles tendonitis, and tennis elbow, all of which involve soft tissue near joints in the distal parts of the body[11]. ART is also effective at reducing pain and increasing ROM in patients with a partial tear of the supraspinatus tendon[12]. Most patients with chronic neck pain experience pain and movement limitation as a result of soft tissue impairment in the neck[13]. Accordingly, more research on ART for the treatment of the soft tissues of the neck is warranted. However, no previous studies have assessed how ART can improve ROM in patients with neck pain.
Therefore, the purpose of this study was to compare the influence of ART and JM on the visual analog scale (VAS) score, pressure pain threshold (PPT), and neck ROM of patients with chronic neck pain, with the aim of elucidating additional information on their effects and identifying more efficient treatments that can be used in clinical settings.
Subjects and Methods
The study subjects were 24 patients admitted to Hospital A in Gangnamgu who had a 3-month or longer history of neck pain and had mild disability based on the Neck Disability Index (NDI; 5–14 points). The sample size of this study was based on that of Hyun[14], while considering the subject dropout rate, and accounting for significance level (5%), power of the test (0.8), and the effect size (f=0.7). Patients with structural abnormalities involving bone fracture or nerves those who had undergone surgery for hernia or had high blood pressure, spondyloarthritis, lumbar spinal stenosis, or scoliosis were excluded from the study. The participating patients understood the study purpose and associated information and provided their written consent to participation. This study was conducted using a procedure ethically suitable for human research in accordance with the Declaration of Helsinki.
We used the VAS to evaluate the degree of neck pain. The VAS is a subjective scoring method for recording the degree of present pain from 0 (no pain) to 10 (the most severe pain ever experienced) on a 10-cm scale. The VAS is difficult to compare among patients because of the subjective nature of the pain, but its reproducibility has been recognized in individual patients (ICC=0.97)[15].
The PPT measurement was performed by one investigator using an algometer. The right and left upper trapezius and sternocleidomastoideus (SCM) were pressed at a constant speed. The subject was asked to respond immediately when the pressure changed to pain, and the mechanical pressure was recorded. The mean value of two measurements was used; increasing PPT values indicate a higher-pressure pain threshold. An algometer is particularly useful for measuring the trigger point in myofacial pain syndrome, because it can determine the precise location of the source pain and quantify the pressure sensitivity of muscles (ICC=0.78–0.93)[16, 17].
Passive ROM was measured by fixing the subject’s shoulder so that it was not affected by the other parts of the trunk. Then, neck flexion, extension, right side bending, left side bending, right rotation, and left rotation were measured. The range of the angle was measured with a therapist passively assessing the patient’s pain-free neck-joint ROM[18].
The 24 subjects with chronic neck pain included in the study were randomly assigned to one of three groups following an equivalent control group pre-test/post-test design. For 3 weeks, the ART and JM groups received treatment twice per week for 20 minutes. After all the interventions were completed, the VAS score, PPT, and ROM were measured again. In the ART group, ART was used to treat the muscles demonstrating scar tissue, among the muscles involved in neck movement. After shortening based on fiber texture in the longitudinal direction, soft tissue mobilization was performed with active or passive stretching to lengthen the tissue that had been shortened[12].
JM was performed using Kaltenborn’s techniques of traction and gliding. In order to relieve pain with physiological movements including flexion, extension, side bending, and rotation, traction at Grade I or II was performed for 10 seconds. Additionally, in order to recover hypomobility, traction and gliding were performed at level 3 and maintained for 7 seconds. Both treatments included 2–3 seconds of rest and were repeated 10 times[19]. Subjects in the control group did not receive any treatment for chronic neck pain.
SPSS 18.0 for Windows was used to analyze the results. In order to confirm the homogeneity of subjects’ general characteristics and dependent variables, descriptive statistics and the Kruskal-Wallis test were used. The Wilcoxon rank test was performed to assess the difference between pre- and post-treatment values in each group, and the Mann-Whitney U test was used to identify significant differences among the groups. The threshold for statistical significance was chosen as 0.05.
Results
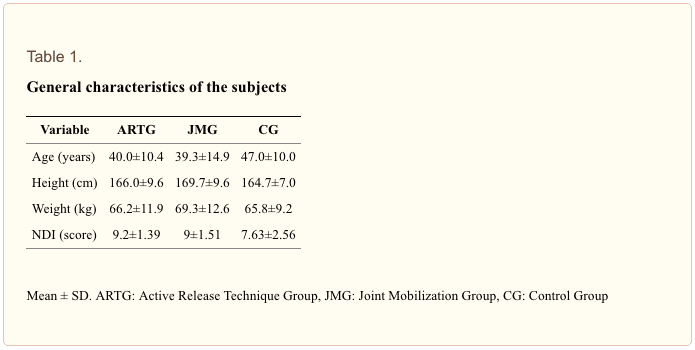
The extent of change in VAS score, PPT, and ROM was compared between patients with chronic neck pain who underwent ART or JM. Twenty-four patients with a 3-month or longer history of chronic neck pain participated in this study. The three groups demonstrated no significant differences in NDI scores, ages, heights, or weights (p>0.05) (Table 1).
The ART and JM groups both demonstrated significant improvements in VAS pain scores (p<0.05), but no significant change was observed in the control group (p>0.05). The PPT significantly increased (p<0.05), in every muscle measured in the ART group, and in all muscles other than the right upper trapezius in the JM group. Muscle PPT demonstrated no significant change in the control group (p>0.05) (Table 2).
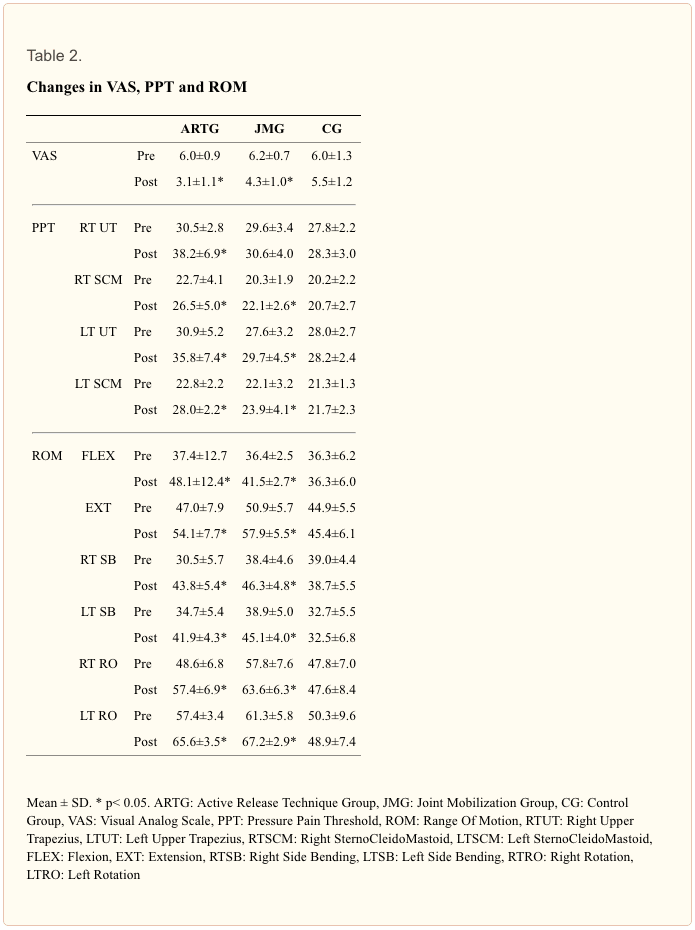
After treatment, the ART and JM groups both demonstrated significant increases (p<0.05) in every neck joint ROM parameter, while no significant changes were observed in the control group (p>0.05) (Table 2).
The extent of change in the VAS pain score and PPT between pre- and post-treatment significantly differed across the three groups (p<0.05). The posthoc test indicated that changes in the VAS scores significantly differed between the ART and control groups, and between the JM and control groups (p<0.05), but not between the ART and JM groups (p>0.05). The changes in PPTs of the right upper trapezius and left SCM significantly differed to between the ART and JM groups (p<0.05); however no significant differences were observed in the other muscles (p>0.05). Between the JM and control groups, the change in right SCM PPT demonstrated a significant difference (p<0.05); however, no difference was observed in other muscles (p>0.05). Between the ART and control group, the change in PPT significantly differed for all the measured muscles (p<0.05). The changes in VAS score and PPT were greater in the ART group than in the JM group, but these differences were not statistically significant (Table 3).
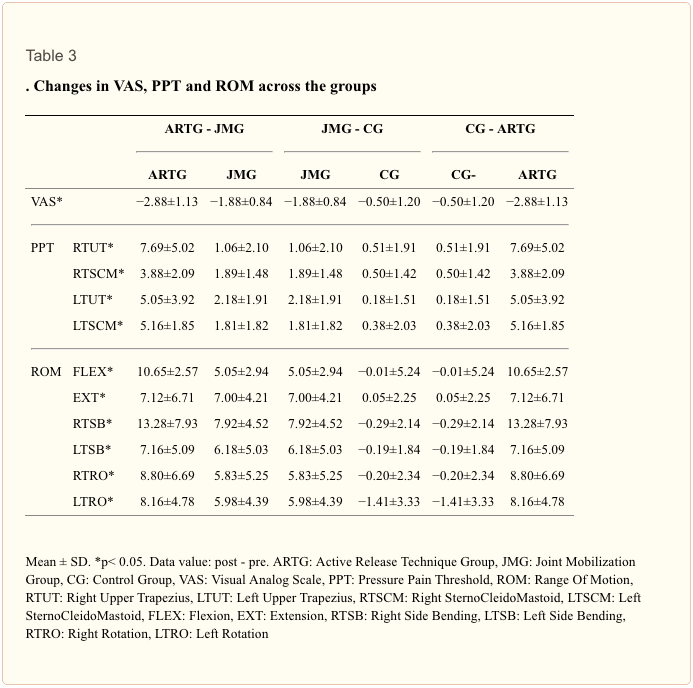
The extent of change in ROM after the treatments significantly differed across the three groups (p<0.05). The posthoc test indicated that the change in ROM significantly differed between the ART and JM groups only in neck flexion (p<0.05), but not in other ROM measurements (p>0.05). There was no significant difference in neck flexion ROM between the JM and control groups (p>0.05), but all other ROM parameters significantly differed between these groups (p<0.05). The ART and control groups significantly differed in terms of the change in ROM for all the parameters measured (p<0.05). The change in ROM was greater in the ART group than in the JM group, but this difference was not reach statistically significant (Table 3).

Dr. Alex Jimenez’s Insight
The following study compared the use of the active release technique (A.R.T.) to the use of joint mobilization to determine the best method for treating chronic neck pain symptoms. As it will be properly described below, the research study concluded that ART and joint mobilizations are both effective as treatment for patients with chronic neck pain, however, the active release technique demonstrated a greater effectiveness for neck pain associated with soft tissue injury. A.R.T. is believed to be a better treatment option for chronic neck pain mainly because soft tissue injuries are believed to be the cause of painful symptoms in 87.5 percent of cases, where ART is performed directly on the area of damage.
Discussion
Repetitive motions and the use of smart phones and tablets in abnormal head postures can stress the head, neck, and shoulder areas. Additionally, abnormal head posture can cause mechanical dysfunction of the cervical joint, which can lead to pain, fibrosis of soft tissue, adaptive shortening, loss of flexibility, and mechanical deformation reflecting the condition of hypomobility, where there is no movement inside the normal joint capsule[20, 21]. When mechanical dysfunction is present in a vertebra, manual therapy is typically performed, and it can be an effective method of relieving neck pain related to such dysfunction[22]. JM is used to treat joints with hypomobility or progressive limitation of mobility, by identifying a cervical segment with abnormal mobility and irritating the sensory receptors that sense pain, thus eliciting effects on the muscle, which in turn stimulate the muscles to apply force in the appropriate direction[8].
After 3 weeks of JM, the VAS, ROM, and PPT values of muscles other than the right upper trapezius demonstrated significant improvements compared to their pre-test values. The PPT also increased in the right upper trapezius, but the difference was not statistically significant. The trapezius is particularly susceptible to damage by repetitive movements of the hand and arm while performing work such as using a computer[23]. Most of the study participants were right-handed and thus performed more movement of the right upper extremity than the left, which may explain why the improvement of the right upper trapezius PPT was not reach statistically significant.
ART is a method for treating the soft tissues such as the tendon, nerve, and myofascia, and is performed for repetitive strain injury, acute injury, and functional fixation damage due to abnormal posture maintained over the long term. Furthermore, ART is an effective at resolving adhesion of scar tissue and the soft tissue that causes pain, spasm, muscle weakness, tingling, and other symptoms[11].
Robb et al.[24] demonstrated immediate improvement of muscle PPT when ART was used to treat patients with adductor strain. Additionally, in a study by Tak et al.[10], ART treatment for 3 weeks on the gluteus medius of a patient with low back pain for 3 weeks resulted in improvement of the patient’s VAS score and PPT. Although our target area differed from the studies of Tak et al.[10] and Robb et al.[24], significant improvement was observed in the VAS score, PPT, and ROM after using ART to treat the neck muscles in the present study. It is our opinion that these improvements in VAS score and PPT after treatment is the result of decreases in muscle tone after removing scar tissue adherent to soft tissue.
In a study by James[25] involving 20 young men with no injury of the lower extremity, hamstring flexibility increased immediately after ART was applied. Similarly, in the present study, ROM significantly increased after ART was applied on the neck for 3 weeks. This finding indicates that scar tissue, which can limit the mobility of soft tissue, can be removed by ART and thus relieve limitations of movement[12].
Although no statistically significant difference was detected in many cases, the change in the VAS score, PPT, and ROM demonstrated a consistent trend toward being greater in the ART group than in the JM group. This greater effect may be related to the observation that soft tissue injury is the cause of pain in 87.5% of neck pain cases, and ART is performed directly on the injured soft tissue[13], whereas JM treats the limited area of the joint. This study compared the effect of treatment over a short period of 3 weeks, and thus, it remains unclear how long its effectiveness is maintained. Longerterm follow-up surveys are needed after the cessation of treatment. Additionally, it is difficult to generalize our findings, as the sample sizes were small. In order to reinforce these findings, more research is needed.
In conclusion, this study compared the VAS score, PPT, and ROM across 24 subjects with chronic neck pain receiving ART, JM, or no treatment. It revealed that ART and JM both positively affected the VAS score, PPT, and ROM, and that the two methods demonstrated few significant differences in their effects. Thus, ART and JM are both effective for the treatment of patients with chronic neck pain, but ART demonstrated a trend toward greater effectiveness for patients with neck pain involving soft tissue injury. Therefore, ART appears to be a better option for treating patients with chronic neck pain in the clinical setting. Follow-up research involving greater numbers and diversity of subjects with longer terms are needed to expand upon these findings.
The purpose of the article above is to present the effectiveness of the active release technique, or ART, towards the management and improvement of chronic neck pain in a clinical setting. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
1. Chung SH, Her JG, Ko TS, et al. : Effects of exercise on deep cervical flexors in patients with chronic neck pain. J Phys Ther Sci, 2012, 24: 629–632.
2. Hwangbo G: Analysis of the change of the neck pressure pain threshold in long term computer users. Int J Contents, 2008, 8: 151–158.
3. Sarig-Bahat H: Evidence for exercise therapy in mechanical neck disorders. Man Ther, 2003, 8: 10–20. [PubMed]
4. Hyung IH, Kim SS, Lee SY: The effect of immediate pain and cervical ROM of cervical pain patients on stretching and manipulation. J Korean Soc Phys Ther, 2009, 21: 1–7.
5. Oh SG, Yu SH: Biomechanical changes in lower quadrant after manipulation of low back pain patients with sacroiliac joint dysfunction. J Korean Soc Phys Ther, 2001, 8: 167–180.
6. Jull GA, Falla D, Vicenzino B, et al. : The effect of therapeutic exercise on activation of the deep cervical flexor muscles in people with chronic neck pain. Man Ther, 2009, 14: 696–701. [PubMed]
7. Ko TS, Jeong UC, Lee KW: Effects of the inclusion thoracic mobilization into cranio-cervical flexor exercise in patients with chronic neck pain. J Phys Ther Sci, 2010, 22: 87–91.
8. Kim DD: The effects of manipulation and mobilization on NDI and CROM in young adults with mild neck disability. J Korean Acad Orthop Man Phys Ther, 2010, 16: 53–60.
9. Jun YW: The effects of upper thoracic joint mobilization technique using Kaltenborn-Evjenth concept on cervicothoracic ROM and pain in patients with chronic neck pain. Graduate school Korea University Master’s Degree, 2012.
10. Tak SJ, Lee YW, Choi W, et al. : The effects of active release technique on the gluteus mediusfor pain relief in persons with chronic low back pain. Physical Therapy Rehabilitation Science, 2013, 2: 27–30.
11. Brian A, Kamali A, Michael Leahy P: Release Your Pain: Resolving Repetitive Strain Injuries with Active Release Techniques. Pub Group West, 2005, 15–29.
12. Lee SJ, Park JH, Nam SH, et al. : Two clinical cases of active release technique with Korean medicine treatment for supraspinatus tendon partial tear. J CHUNA Man Med Spine Nerves, 2014, 9: 89–101.
13. Dvord J, Valach L, Schmdt S: Cervical spine injuries in Swizerland. Man Med, 1989, 4: 7–16.
14. Hyun SW: The effects of joint mobilization and conservative physical therapy on the range of motion and pain in patients with cervical pain. Graduate school Kookmin University Master’s Degree, 2003.
15. Bijur PE, Silver W, Gallagher EJ: Reliability of the visual analog scale for measurement of acute pain. Acad Emerg Med, 2001, 8: 1153–1157. [PubMed]
16. Kim SH, Kwon BA, Lee WH: Effects of cervical spinal stabilization training in private security on chronic neck pain and cervical function, neck pain, ROM. Korean Secur Sci Rev, 2010, 25: 89–107.
17. Cho SH: The effect of myofascial release technique and forward head posture correction exercise on chronic tension-type headache. Graduate school Catholic University of Pusan Doctor’s Degree, 2014.
18. Jang HJ: Effects of combined exercise program on pain and function and range of motion and fatigability in chronic neck pain. Graduate school University Sahmyook Master’s Degree, 2011.
19. Kim HJ, Bae SS, Jang C: The effects of joint mobilization on neck pain. J Korean Soc Phys Ther, 2003, 15: 65–90.
20. Côté P, Cassidy JD, Carroll LJ, et al. : The annual incidence and course of neck pain in the general population: a population-based cohort study. Pain, 2004, 112: 267–273. [PubMed]
21. Lee JH, Lee YH, Kim HS, et al. : The effects of cervical mobilization combined with thoracic mobilization on forward head posture of neck pain patients. J Phys Ther Sci, 2013, 25: 7–9.
22. Ferreira LA, Santos LC, Pereira WM, et al. : Analysis of thoracic spine thrust manipulation for reducing neck pain. J Phys Ther Sci, 2013, 25: 325–329.
23. Seo HK: The effect of myofascial release, joint mobilization, and Mckenzine on the cervical muscle activity. Graduate school Daegu University Doctor’s Degree, 2008.
24. Robb A, Pajaczkowski J: Immediate effect on pain thresholds using active release technique on adductor strains: pilot study. J Bodyw Mov Ther, 2011, 15: 57–62. [PubMed]
25. George JW, Tunstall AC, Tepe RE, et al. : The effects of active release technique on hamstring flexibility: a pilot study. J Manipulative Physiol Ther, 2006, 29: 224–227. [PubMed]

Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.

Post Disclaimer
Professional Scope of Practice *
The information on this blog site is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those found on this site and our family practice-based chiromed.com site, focusing on restoring health naturally for patients of all ages.
Our areas of chiropractic practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is limited to chiropractic, musculoskeletal, physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system.
Our videos, posts, topics, subjects, and insights cover clinical matters and issues that relate to and directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: coach@elpasofunctionalmedicine.com
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License # TX5807
New Mexico DC License # NM-DC2182
Licensed as a Registered Nurse (RN*) in Texas & Multistate
Texas RN License # 1191402
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card